
Community Health Needs Assessment and
Implementation Strategy Report
2019-2021

Montefiore St. Luke’s Cornwall
Community Health Needs Assessment and Implementation Strategy Report 2019-21
Table of Contents
Item
Page Number
Executive Summary
Pages 2-3
The 2019-2021 CHNA
Introduction
• Organizational Background
• Statement of Executive Review
• Date report is made available to the public
Pages 4- 5
CHNA Process and Methods
• Description of the process and methods used to conduct the
assessment
• Involved Personnel
• Description of Planned Approach
o analytical methods used to identify the community health
needs
o description of statistical tests or processes
Pages 5-6
Input Representing the Broad Interests of the Community
• Stakeholders and partners that participated in the prioritization
process
• Methodology for selection including group consensus processes
• Comments received on the hospital facility’s most recently conducted
CHNA and most recently adopted implementation strategy
Pages 6-7
Definition/Description of the Community Service Area
• Description of the population/community served by the hospital
facility
• Unique community characteristics/resources
Pages 7- 21
Primary Data Collection Plan
• Data and information sources for primary data collection
• Description of type of methodology (interviews, survey, focus group)
• Rationale for methodology selection
• Setting(s) of primary data collection
o Specific target populations response rate by setting and
population (number interviewed, numerator and denominator
of surveys sent and returned — include percentage and actual
numbers)
o Description and list of successful approaches and
identification
o Description and list of barriers, challenges and unsuccessful
approaches
Pages 21-24
Secondary Data Collection Plan
• Data and information sources for secondary data
Pages 24-26

o agency or organization
o retrieval date
o year of data available and used
o Web address
o rationale for use of these data sources
Primary Data Collection Plan
• Data and information sources for primary data collection
• Description of type of methodology (interviews, survey, focus group)
• Rationale for methodology selection
• Setting(s) of primary data collection
o Specific target populations response rate by setting and
population (number interviewed, numerator and denominator
of surveys sent and returned — include percentage and actual
numbers)
o Description and list of successful approaches and
identification
o Description and list of barriers, challenges and unsuccessful
approaches
Presentation of Data
• Overview (Maps)
Pages 26-41
Review of Key Findings
• Summary List of Specified Community Needs
Pages 41-46
Special Considerations
• Gaps in information that limited the ability to assess the community
served
• Description and list of specific gaps
Page 46
Implementation Strategy Report
Pages 47-48
Significant Needs to Be Addressed
• Anticipated impact of those actions
• Description of resources available to address the health need
• Planned collaborations with other facilities or organizations
Pages 47-48
Significant Needs Not Addressed
• Explanation of rationale
• Anticipated impact of those actions
• Description of alternate resources available to address the health
need
Pages 48-49
Appendix
• Regional Community Health Assessment Survey
• Stakeholder Interview Form
Pages 50-55
Pages 56-58
2
EXECUTIVE SUMMARY
Monteore St. Luke’s Cornwall (MSLC), a formal member of the Monteore Health System, is a not-for-prot community
hospital with campuses in Newburgh and Cornwall, NY, as well as several o-site facilities, that provides dedicated care to
more than 250,000 patients per year. MSLC is a 242-bed acute care hospital with a geographic coverage area that serves a
population of approximately 400,000 people. As a safety net and Vital Access Provider, MSLC serves a population that has been
designated as a medically underserved area (MUA), specically in the City of Newburgh.
The Monteore St. Luke’s Cornwall Community Health Needs Assessment was compiled using specic data provided from the
Mid-Hudson Region Community Health Assessment 2019-2021, which was MSLC’s Primary Data Collection Source. The Mid-
Hudson Region Assessment Community Health Assessment 2019-2021, originated from a Collaborative that was formed in
2017 from the seven local health departments across the Mid-Hudson Region, with a goal of creating the rst ever regional
community health survey. These counties include Dutchess, Orange, Ulster, Putnam, Sullivan, Rockland and Westchester. There
were 17 local hospitals who contributed funds for the Collaborative to contract with the Siena College Research Institute, to
conduct a randomized, digital-dial community health survey. The survey captured a total of 5,372 responses and roughly 850
from Orange County specically, which would supplement the Regional Community Health Assessment. In addition to the
phone survey, several Provider Focus Groups formed a collaborative with Human Service providers throughout the region.
Prior to the focus groups, a survey was sent to providers in each county in an eort to supply additional background regarding
local factors that inuence community health. The survey was inclusive of the populations that are served by the providers,
issues that impact those communities, barriers that exist in helping residents achieve better health and the interventions used
to address the social determinants of health. A total of 285 surveys were completed by the service providers, with a total of 41
responses from Providers in Orange County.
The Human Service Provider Survey and Focus Groups identied that the top-rated issues aecting health in Orange
County are:
1) Access to aordable, decent and safe housing
2) Access to aordable, reliable, personal and public transportation
3) Access to mental health providers
Additionally, the above ndings revealed that the top three barriers in achieving better health in Orange County
include:
1) Knowledge of existing resources
2) Drug and/or alcohol use
3) Healthy literacy
The Mid-Hudson Region Community Health Assessment ndings indicated that in Orange County, Heart Disease and Cancer
are among the leading causes of death and leading causes of premature death (death before age 75) by a large margin.
Obesity is a leading contributor to these top causes of death, as well as diabetes, stroke, and hypertension—all of which
can lead to premature death. Over the past ten years, the rates of obesity have continually grown, as well as the subsequent
morbidity of cardiovascular disease, prediabetes, and hypertension.
Sexually Transmitted Infections are also signicantly on the rise in Orange County. There has been a 75% increase in the
average number of newly diagnosed HIV cases in Orange County from 17.2 per year (2011-2015) to 26.3 per year (2016-2018).
Chlamydia rates among both males and females from 2014-2016 are higher in Orange County than rates in the Mid-Hudson
Region, and have steadily increased or remained the same from 2011-2013 to 2014-2016. Additionally, Orange County had its
rst fetal demise in 2019 from congenital syphilis in over 25 years.
In addition to our contributions in the Mid-Hudson Region Community Health Assessment 2019-2021, MSLC also participated
in the Orange County Health Summit in June 2019, as part of a secondary data collection process. This summit served as an
active working session to review the data from the above-mentioned Provider focus groups, along with the Siena College
Survey Data, and ultimately decide on the Priority Areas for the 2019-2021 Community Health Improvement and Community
Service Plan.
3
The two Prevention Agenda Priorities that Orange County selected at this summit are:
• Prevent Chronic Disease
• Prevent Communicable Disease
The two priority areas that Monteore St. Luke’s Cornwall has identied as a result of the Community Health Needs
Assessment and the discussion at the Orange County Community Health Summit are the same: Prevent Chronic Disease and
Prevent Communicable Disease. These ndings were used to help create the 2019-2021 Community Service Plan.
Date Report is Made Available to the Public: The 2019 Community Needs Assessment will be submitted on December 30,
2019 and will be posted to the hospital’s website https://www.monteoreslc.org/community/community-service-plan/.
This report was approved by the Monteore St. Luke’s Cornwall Board of Trustees on Tuesday, November 26, 2019.

4
INTRODUCTION
Organizational Background
Monteore St. Luke’s Cornwall (MSLC), a formal member of Monteore Health System, is a not-for-prot community hospital
with campuses in Newburgh and Cornwall, NY, as well as several o-site facilities, that provide dedicated care to more than
250,000 patients per year.
MSLC is a 242-bed acute care hospital with a geographic coverage area that serves a population of approximately 400,000
people. As a safety net provider, MSLC serves a population that has been designated as a medically underserved area (MUA),
specically in the City of Newburgh.
MSLC’s Newburgh campus is comprised of both inpatient and outpatient services including a Level III Trauma Center,
Emergency Department, Intensive Care Unit, Cardiac Catheterization Laboratory, Birthing Center and Neonatal Intensive Care
Unit, Physical Therapy as well as surgical services including Orthopedics, Urology and Men’s Health procedures, Metabolic
and Bariatric Surgery, and Oncology. The Cornwall campus has shifted to an entirely outpatient model in the last ten years,
and includes the Littman Cancer Center, an Infusion Suite, Center for Pain Management, Center for Sleep Medicine, Center for
Wound Care and Hyperbaric Medicine, Laboratory, and Rehabilitative Services, inclusive of Physical, Occupational and Speech
Therapies, along with Cardiac and Pulmonary Rehabilitation, and most recently a Center for Cognitive and Memory Services
and a Driver Evaluation and Advisement Program.
Inpatient Discharges specic to Monteore St. Luke’s Cornwall
The Top 20 inpatient discharges for Monteore St. Luke’s Cornwall’s Newburgh campus in 2018 are shown below, with the
highest percentage being Sepsis, liveborn infants according to place of birth and type of delivery, along with pneumonia,
unspecied organism, and osteoarthritis of the knee. These discharges show the direct correlation between the health
disparities and barriers that exist among the population that MSLS services and the types of conditions the hospital treats
most frequently.
Table X. Top 20 inpatient discharges at Monteore St. Luke’s Cornwall-Newburgh (formerly St. Luke’s Cornwall Hospital), 2018
A41 Other sepsis 905 8.3%
Z38 Liveborn infants according to place of birth and type of delivery 904 8.3%
J18 Pneumonia, unspecied organism 370 3.4%
M17 Osteoarthris of knee 337 3.1%
J44 Other chronic obstrucve pulmonary disease 276 2.5%
N17 Acute kidney failure 272 2.5%
I21 Acute myocardial infarcon 250 2.3%
L03 Cellulis and acute lymphangis 208 1.9%
E11 Type 2 diabetes mellitus 202 1.8%
I11 Hypertensive heart disease 202 1.8%
I13 Hypertensive heart and chronic kidney disease 162 1.5%
M16 Osteoarthris of hip 160 1.5%
I48 Atrial brillaon and uer 152 1.4%
I63 Cerebral infarcon 151 1.4%
S72 Fracture of femur 148 1.4%
K85 Acute pancreas 134 1.2%
O99
Other maternal diseases classiable elsewhere but complicang
pregnancy, childbirth and the puerperium 134 1.2%
O34 Maternal care for abnormality of pelvic organs 131 1.2%
E87 Other disorders of uid, electrolyte and acid-base balance 124 1.1%
N39 Other disorders of urinary system 121 1.1%
- Other diagnoses 5,577 51.1%
Data source: Internal Monteore Health System data, 2018
ICD-10 Code Label Discharges % of total

5
STATEMENT OF EXECUTIVE REVIEW:
Monteore St. Luke’s Cornwall (MSLC) has participated in an extensive Community Health Needs Assessment which is outlined
throughout this document. The CHNA includes data from the Mid-Hudson Regional Community Health Assessment 2019-
2021, which is inclusive of data from the Mid-Hudson Region Community Health Survey, and Provider Focus Groups. The
Mid-Hudson Regional Community Health Assessment which was written by HealtheConnections with contributions and input
from many partners throughout the Mid-Hudson Region. Additionally, MSLC participated in the June 2019 Orange County
Community Health Summit, and a number of focus groups that were created as a result of the summit.
This document outlines the overview of the population MSLC serves, the primary health disparities, barriers to accessing care,
and the key ndings of the surveys MSLC has participated in.
The two priority areas that Monteore St. Luke’s Cornwall has identied as a result of the Community Health Needs
Assessment are the following: Prevent Chronic Disease and Prevent Communicable Disease. These ndings were used to
help create the 2019-2021 Community Service Plan.
Date Report is Made Available to the Public:
This document will be made available to the public on December 30, 2019, via the Hospital’s website at www.MonteoreSLC.org.
COMMUNITY HEALTH NEEDS ASSESSMENT PROCESS AND METHODS
To assess the broad interest of the community, Monteore St. Luke’s Cornwall participated in the Mid-Hudson Regional
Community Health Assessment 2019-2021, also referred to as the Siena College survey, which was compiled and written by
HealtheConnections and inclusive of data pertaining to the seven counties within the Mid-Hudson Region. This assessment
originated from a collaborative that was formed in 2017 from the seven local health departments across the Mid-Hudson
Region, with a goal of creating the rst ever regional community health survey. These counties include Dutchess, Orange,
Ulster, Putnam, Sullivan, Rockland and Westchester. There were 17 local hospitals who contributed funds for the Collaborative
to contract with the Siena College Research Institute, to conduct a randomized digital dial community health survey, which
would supplement the Regional Community Health Assessment.
Involved personnel:
The above-mentioned Collaborative Consists of the following hospitals and health systems:
• Bon Secours Charity Health System, a member of the Westchester Medical Center Health Network
• Good Samaritan Hospital
• Bon Secours Community Hospital
• St. Anthony Community Hospital
• Dutchess County Department of Behavioral & Community Health
• Catskill Regional Medical Center, a member of the Greater Hudson Valley Health System
• HealthAlliance Hospitals, members of the Westchester Medical Center Health Network
• Nuvance Health:Northern Dutchess Hospital
o Vassar Brothers Medical Center
o Putnam Hospital Center
• Monteore Health System
• Monteore Hudson Valley Collaborative
• Monteore Nyack Hospital
• Monteore St. Luke’s Cornwall
• Orange County Department of Health
• Orange Regional Medical Center, a member of the Greater Hudson Valley Health System
• Putnam County Department of Health
• Rockland County Department of Health
• St. Joseph’s Medical Center
• Sullivan County Public Health Services
• Ulster County Department of Health and Mental Health
• Westchester County Department of Health

6
This Survey was titled the Mid-Hudson Region Community Health Survey. A total of 5,372 residents across the Mid-Hudson
Region were surveyed, which breaks down to approximately 767 responses per county. The survey was crafted with questions
that would collect information regarding the varying priorities and initiatives put forth by the New York State Department
of Health. Among these were The Prevention Agenda, The Eight Domains of Livability, and incorporating healthy aging into
Health Across all Policies.
Each of the seven counties were divided into two specic regions chosen by the Local Health Departments and then half of
the surveys from each county were collected in each region. The Collaborative then retained SCRI to conduct a digital dial
survey by phone at random. The telephone surveys were conducted between April and September 2018 and included both
landline and cell phone numbers to reach a variety of respondents. The results were weighted by age, gender, race and region
according to the U.S. Census 2010. A sample of the Survey questions is provided in Appendix A.
The Demographic Breakdown of Respondents is shown in the table below:
Key Findings from the Community Health Survey included:
• 81% of Orange County respondents reported that accessible and convenient transportation was “very important” or
“somewhat important” to them
• 80% of Orange County respondents reported that people may have a hard time nding a quality place to live due to
the high cost of living
• 39% of Orange County respondents living in rural areas reported that places in Orange County did not feel safe vs.
54% of Orange County respondents living in urban zip codes
• 27% of Orange County respondents with <$25K yearly income reported experiencing a mental health condition or
substance or alcohol use disorder compared to 14% of total Orange County respondents
• 28% of Orange County respondents with <$25K yearly income reported that in the past 12 months, they or any other
member of their household has been unable to get food compared to 11% of total Orange County respondents
• 35% of Orange County respondents with <$25K yearly income reported that in the past 12 months, they or any other
member of their household has been unable to get medicine compared to 14% of total Orange County respondents
Input Representing the Broad Interest of the community
To further assess the broad interests of the community, following the Regional Assessment. Several focus groups were
created to gain the insights of the underrepresented populations in the community, including those who are seniors, low
income, veterans, LGBTQ members, those experiencing homelessness, and residents with a mental health diagnosis. 12
focus groups, with members of the providers who serve these populations were created collaboratively with Human Service
providers throughout the region. Prior to the focus groups, a survey was sent to providers in each county in an eort to supply
additional background regarding local factors that inuence community health. The survey was inclusive of the populations
that are served by the providers, issues that impact the communities the providers serve, barriers that exist in helping
residents achieve beer health and the intervenons used to address the social determinants of health. A total of 285 surveys
were completed by the service providers, with varying answers in each county. The dierences were then discussed at length in
each of the focus groups. A sample of the interview form is provided in Appendix B.

7
In Orange County specically, a total of 41 responses were collected from providers that serve a variety of populaons.
According to the Mid-Hudson Regional Community Health Assessment, The Orange County Department of Health, joined by
HealtheConnecons, conducted a focus group at the Joint Membership of Health and Community Agencies (JMHCA), with a
focus on providing the residents of Orange County with a comprehensive plaorm for health and wellness. Several agencies
were represented in this meeng, and the discussion was centered around the survey quesons that were distributed prior to
the focus group. The providers involved in the focus groups, serve a diverse group of clients including children and adults with
disabilies, those with substance abuse disorders, and low-income individuals. The types of residents that these providers serve
is shown in Appendix C.
Comments received on the most recently conducted Community Health Needs Assessment address areas of concern that
Monteore St. Luke’s Cornwall specically had when creang this document, specically that MSLC’s Primary Service Area,
inclusive of the City of Newburgh is not well reected in this data. The nal Mid-Hudson Region Community Health Assessment
2019-2021, notes that while the results give an extensive background on the health needs of the
Mid-Hudson region, the nal results are misleading and mask several of the disparities that exist in the Urban areas of Orange
County specically. The nal assessment states: At rst glance, Orange County appears to be an auent suburban community
that enjoys a median household income above the New York State average ($75,146 vs. $62,765, respectively); a smaller percentage
of individuals living below the poverty line (12.2% vs. 15.1% respectively); a smaller unemployment rate (5.6% vs. 6.6%, respectively);
and boasts a higher percentage of high school graduates as compared to New York State (89.6% and 86.1%, respectively). However,
aggregate county data are misleading and masks the disparities within the County. The urban areas of Orange County are
characterized by severe socioeconomic and health inequities, with one-third of the population living below the poverty line and
residing in the three major cities (Newburgh, Middletown, and Port Jervis).
Denition and Description of the Community Service Area
Monteore St. Luke’s Cornwall (MSLC) is a not-for-prot community hospital with campuses in Newburgh and Cornwall, NY, as
well as several o-site facilities, that provide dedicated care to more than 250,000 patients per year. MSLC is a 242-bed acute
care hospital with a geographic coverage area that serves a population of approximately 400,000 people. As a safety net and
Vital Access Provider, MSLC serves a population that has been designated as a medically underserved area (MUA), specically
in the City of Newburgh.
MSLC’s Primary Service Area is comprised of 12 neighboring zip codes, with nine of the twelve zip codes residing in Orange
County, two in Ulster County and one in Dutchess County.
The Mid-Hudson Region is comprised of seven counties including Dutchess, Orange, Putnam, Rockland, Sullivan, Ulster
and Westchester. Orange County is roughly 40 miles north of New York City and resides between the Delaware River in the
west and the Hudson River in the east. Orange County is bordered by both New Jersey and Pennsylvania on the southwest.
Orange county is 839 square miles and is comprised of a suburban, rural, urban and farmland areas, which include three cities
(Middletown, Newburgh and Port Jervis), which make up close to 18% of the population of the entire county. Specically,
Newburgh falls in Monteore St. Luke’s Cornwall’s Primary Service Area and is a key focus throughout this entire document.

8
Orange County is also inclusive of 20 towns and 19 villages, 19 school districts along with three colleges and universities, one
of which resides in MSLC’s Primary Service Area, in the heart of the city of Newburgh: Mount Saint Mary College.
The City of Newburgh is the most densely populated portion of MSLC’s Primary Service Area, with roughly 28,444, according
to the American Community Survey 5-year estimates (2013-2017). This same survey indicates that there are 7,473.3 people per
square mile in the City of Newburgh.
(Source: https://censusreporter.org/proles/16000US3650034-newburgh-ny/)
Adults ranging from 35-64 years of age makeup the majority of the population in Orange County.

9
The median age in the City of Newburgh is 27.9 years with 52% of the population being females.
The overall population of the Mid-Hudson Region was split fairly evenly between males and females according to the Mid-
Hudson Regional Community Health Assessment, with data stratied from the U.S. Census Bureau, 2017 American Community
Survey 5 year estimates.
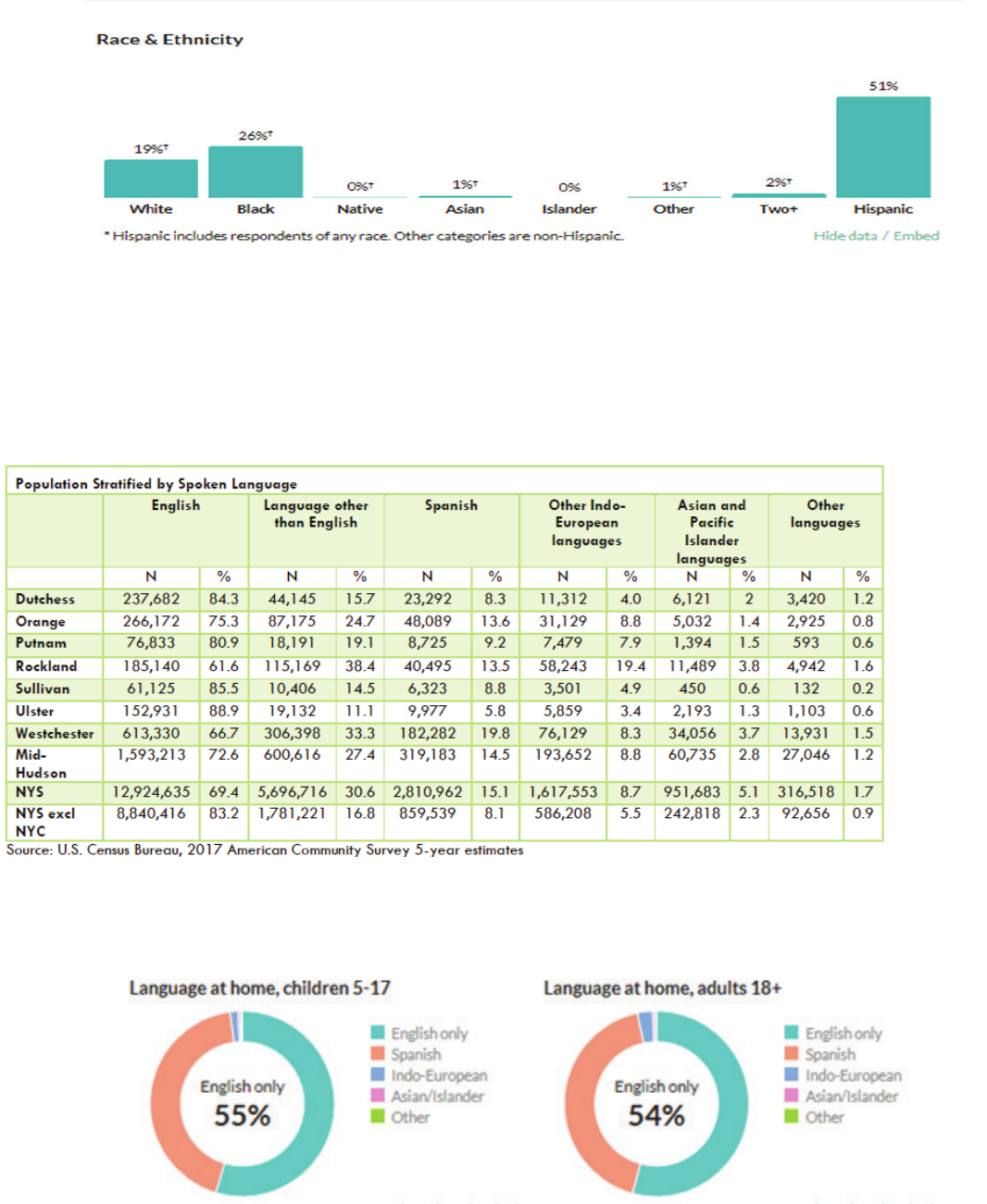
Furthermore, Orange County’s population is 65.4% non-Hispanic White, with the second largest group being Hispanic at
19.7%. However, in the City of Newburgh, the largest population broken down by race/ethnicity is Hispanic, at 51%.
10
In the City of Newburgh, more than half of the population speak only English at home. Spanish is the second most commonly
spoken language at home.
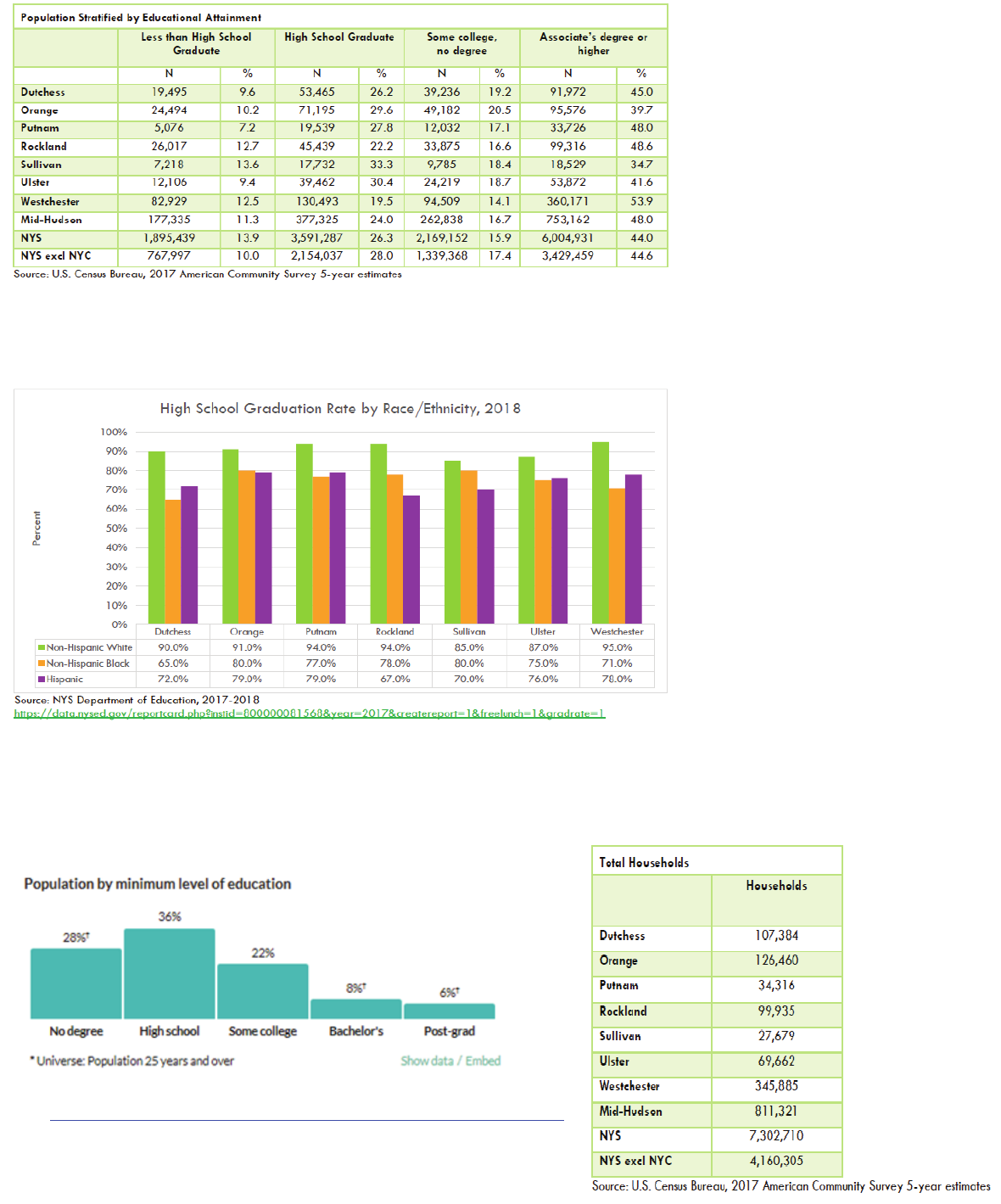
Of those ages 25 years or older, more than 240,447 residents in Orange County have attained an Associate degree or higher.
Across the Mid-Hudson Region, Westchester had the highest percentage (53.9%) and Sullivan County the lowest (34.7%). Only
39.7% of Orange County residents had an Associate degree or higher.
Source:
https://censusreporter.org/proles/16000US3650034-newburgh-ny/
The Mid-Hudson Region Community Health Assessment 2019-2021 indicates that the most commonly spoken language in
Orange County is English at 75.3%.
11
The Mid-Hudson Regional Community Health Assessment 2019-2021 shows that across all counties in the region, White students
had a higher graduation rate than Hispanic and Non-Hispanic Black students.
City of Newburgh educational attainment rates were far worse. Six percent of City of Newburgh residents have attained an
associate degree, and roughly 36% of the population has achieved a high school or equivalent degree.
Source: https://data.census.gov/cedsci/prole?hidePreview=true&g=1600000US3650034
The 2019 Mid-Hudson Regional Community Health Assessment indicates
that 37.1% of Orange County residents had an annual income of greater
than $100,000. The total households accounted for in this overall estimate
was 126,640 in Orange County.

12
In the City of Newburgh, only 14% of residents have an annual income of greater than $100,000, with a median household
income of $36,922 and 31.2% of the population below the poverty line.
Source: https://data.census.gov/cedsci/prole?hidePreview=true&g=1600000US3650034
Orange County as a whole had a 9.1% rate of families below the poverty line, which was the fourth highest rate in the Mid-Hudson Region,
with Sullivan being the highest at 12.5%
Employment plays a large role in one’s health. The Mid-Hudson Region Community Health Assessment indicates that there is a 5.6%
unemployment rate in Orange County.

13
The most common mode of transportation to work across the county was via car, alone.
The most common mode of transportation to work for City of Newburgh residents is also by car.

14
Disability:
A disability adjusted life year is considered to be a summary measure of population-health that combines data on premature
mortality and disability to identify the leading causes of ill health. The causes of disability adjusted life years in New York State, in
all ages and both sexes include COPD, Diabetes, Depression, Stroke, Lung Cancer, Breast Cancer, Colorectal Cancer, Drugs, Falls,
HIV and much more, according to the Orange County CHNA/CSP Data Dashboards provided by Monteore Health System.
Risk factors for disability adjusted life years in New York State include High Body Mass Index, Dietary Risks, Tobacco, High
Fasting Plasma Glucose, High Blood Pressure, Drug Use, Alcohol Use, Malnutrition and many other factors (see below).
15
The list of measures includes:
• Poverty
• Health insurance status
• Regular PCP
• Fall hospitalizations
• Assault-related hospitalizations
• Adult obesity
• Child obesity
• Adult smoking
• Asthma ED visits
• Diabetes hospitalizations
• CRC screening
• CRC incidence*
• Breast cancer incidence* (Not included in New York State PA dashboard, but alternative sources exist)
• Child immunizations
• Flu immunizations
• HIV incidence
• Chlamydia
• Preterm births
• Breastfed in hospital
• Adolescent pregnancy
• Poor mental health
• Binge drinking
• Suicide rate
• Opioid burden rate*(Not included in New York State PA dashboard, but alternative sources exist)
The Mid-Hudson Regional Health Assessment 2019-2021, references that in New York State roughly one in four adults (more
than 3.3 million people) are living with a disability. The World Health Organization denes this as “disabilities can aect three
dimensions of life: impairment to body structure or mental function, activity limitation, such as diculty hearing, moving or
problem solving; and participation restrictions in daily activities, such as working, engaging in social or recreational activities
or accessing healthcare or preventative services. Its noted that adults with a disability commonly have a higher rate of chronic
health conditions, including diabetes, heart disease and obesity.
The types of disabilities outlined in the Community Needs Assessment include:
• Independent living disability – diculty performing tasks or errands alone, such as visiting a doctor’s oce or shopping
due to a physical, mental, or emotional condition
• Cognitive disability – serious diculty concentrating, remembering, or making decisions due to a physical, mental, or
emotional condition
• Self-care disability – diculty handling tasks, such as dressing or bathing on one’s own
• Mobility disability – diculty moving around physically, such as walking or climbing stairs
• Hearing disability – deafness or serious diculty hearing
• Vision disability – blindness or serious diculty seeing (even when wearing glasses)

16
According to the Mid-Hudson Region Community Health Assessment Orange County had the highest rate of adults living with
a self-care disability (4.8%), and the second highest rate of adults living with any disability (25.9%).
According to the US Census Bureau, 12.5% of the population of the City of Newburgh is disabled.
Source: https://data.census.gov/cedsci/prole?hidePreview=true&g=1600000US3650034
Source: https://data.census.gov/cedsci/prole?hidePreview=true&g=1600000US3650034
Access to healthy food largely impacts one’s ability to lead a healthy lifestyle. Those who are faced with food insecurity, often
make the choice between food, medical care, housing and utilities. The Mid-Hudson Regional Community Health Assessment
notes that other populations who are more vulnerable to food insecurity than the overall population include:
• Senior Populations
• Those living in rural communities
• Black Populations
• Hispanic Populations
• Those living in poverty
Orange County has an 8.5% overall rate of food insecurity, and 16.6% rate of food insecurity among children.
Orange County was also among the lowest density rate of grocery stores per population, at 28.7 per 10,000.

17
As noted in the Mid-Hudson Region Health Assessment 2019-2021, the National School Lunch Program is a federal program
that provides free, nutritionally balanced lunches to children each school day. While Sullivan County had the highest rate of
students eligible for free and reduced lunch in 2016-2017, Orange County had 32% of students eligible for free lunch, and 5%
eligible for reduced price lunch.
The Newburgh Enlarged City School District provides free breakfast and lunch to all students as part of a federally funded
grant program. The district website indicates: Students in the Newburgh Enlarged City School District will begin the 2017-18
school year on the right track with free nutritious meals in school. The Community Eligibility Provision (CEP) provides an opportunity
for districts in high poverty areas to provide free breakfast and lunch to all students without the encumbrance of collecting and
processing school meal applications for free and reduced-price meals. In addition, Community Eligibility allows families to reallocate
the money previously used for the lunch program back into supporting their household.
The Mid-Hudson Region Community Health Survey revealed that Orange County had the lowest rate of respondents who
reported eating a balanced healthy diet all 7 days in an average week over the past 12 months.
Also, of note, 5.0% of the population of Orange County has limited access to Healthy Foods. While specic data was not available
in the same breakdown, these rates are far worse in the City of Newburgh, located within MSLC’s Primary Service Area.

18
Six percent of Orange County Residents overall were uninsured in 2016. This number is also believed to be far higher in areas of MSLC’s
Primary Service Area, specically the City of Newburgh population but exact data was not available.
Additionally, 11% of Orange county respondents indicated being unable to get food when it was really needed.
Access to healthcare providers is another social determinant identied in the Mid-Hudson Region, and is specically a
challenge in the City of Newburgh due to limited access to transportation, and the cost of care/no insurance, among other
items.
The Mid-Hudson Region Community Health Assessment 2019-2021 notes that 11.1% of Orange County residents did not receive
medical care due to cost in 2016. While Orange County may not be among the highest, the numbers are far higher in the City
of Newburgh as compared to the county as a whole.

19
Access to the ratio of providers to population also has an impact on the residents of the Mid-Hudson Region, as noted in the
areas of Mental Health Professionals, Dental Health Professionals and Primary Care providers.
Orange County had the second lowest rate of respondents indicating that in the past 12 months, the respondent or a member
of their household was unable to get any healthcare including Dental or Vision when it was really needed.
The Mid-Hudson Region Community Health Assessment notes that the health professional shortage rates are among the highest in
Orange and Westchester Counties.
92% of respondents in the Mid-Hudson Region Community Health Survey reported having health insurance, and of those, 37% are
getting their insurance through their employer. Of note, 9% of respondents in Orange County have Medicaid as their insurance, and
19% Medicare. MSLC’s overall payer mix in 2018 is 77.8% government payer mix and 19% charity care.

20
The results of the Mid-Hudson Region Community Health Survey reveal that 82% of Orange County residents report having
visited a primary care physician for a routine physical or checkup within the last 12 months.
Furthermore, specic responses from the 850 Orange county residents as part of the Mid-Hudson Region Community Health
Survey indicates that of those who did not visit a primary care physician in the last 12 months, 14% responded the cause was due
21
Unique Characteristics of Orange County’s direct population that Monteore St. Luke’s Cornwall serves include the following:
• A higher than average rate of unemployment as compared to Orange County
• A lower degree of educational attainment as compared to Orange County
• More than 30% of the population is living below the poverty line
• The rate of obesity in adults has increased since 2009 in both adults and school aged children
• The rate of Cardiovascular Diseases in the Hudson Valley is among the highest in Orange County and even higher than the
New York State average.
• The hypertension hospitalization rate in Orange County is higher than the average throughout the Hudson Valley and
New York State as a whole.
• Mortality rates from Cardiovascular Disease in Orange County are also above both Hudson Valley and New York State rates
(223.4 per 100,000).
• Orange County residents are faced with limited access to supermarkets and other sources of healthy and aordable foods.
• Dened as a low-income census tract with at least 500 people, or 33 percent of the population, living more than 1 mile
(urban areas) or more than 10 miles (rural areas) from the nearest supermarket, supercenter, or large grocery store
• Orange County has a higher percentage of residents (4.9%) tting the criteria outlined above than the Hudson Valley rate
and New York State overall
• There has been a signicant increase (75%) in the average number of newly diagnosed HIV cases in Orange County from
17.2 per year (2011-2015) to 26.3 per year (2016-2018)
Primary Data Collection
Monteore St. Luke’s Cornwall’s primary data source was the Mid-Hudson Region Community Health Assessment 2019-
2021, which includes a total of 5,372 residents across the Mid-Hudson Region, which breaks down to approximately 767
responses per county. The survey was crafted with questions that would collect information regarding the varying priorities
and initiatives put forth by the New York State Department of Health. Among these were The Prevention Agenda, The Eight
Domains of Livability, and incorporating healthy aging into Health Across all Policies.
Each of the seven counties were divided into two specic regions chosen by the Local Health Departments and then half of
the surveys from each county were collected in each region. The Collaborative then retained SCRI to conduct a digital dial
survey by phone at random. The telephone surveys were conducted between April and September 2018 and included both
landline and cell phone numbers to reach a variety of respondents. The results were weighted by age, gender, race and region
according to the U.S. Census 2010. A sample of the Survey questions is provided in Appendix A.
In addition to the Mid-Hudson Regional Community Health Survey, several focus groups were created to gain the insights of
the underrepresented populations in the community, including those who are seniors, low income, veterans, LGBTQ members,
those experiencing homelessness, and residents with a mental health diagnosis. In an eort to ensure that the needs of
the underrepresented were addressed, 12 focus groups, with members of the providers who serve these populations were
created. collaborative with Human Service providers throughout the region. Prior to the focus groups, a survey was sent
to providers in each county in an eort to supply additional background regarding local factors that inuence community
health. The survey was inclusive of the populations that are served by the providers, issues that impact the communities the
providers serve, barriers that exist in helping residents achieve better health and the interventions used to address the social
determinants of health. A total of 285 surveys were completed by the service providers, with varying answers in each county.
The dierences were then discussed at length in each of the focus groups. A sample of the interview form is provided in
appendix B
In Orange County specically, a total of 41 responses were collected from providers that serve a variety of populations.
According to the Mid-Hudson Regional Community Health Assessment, The Orange County Department of Health, joined by
HealtheConnections, conducted a focus group at the Joint Membership of Health and Community Agencies (JMHCA), with a
focus on providing the residents of Orange County with a comprehensive platform for health and wellness. Several agencies
were represented in this meeting, and the discussion was centered around the survey questions that were distributed prior to
the focus group.
22
The providers involved in the focus groups, serve a diverse group of clients including children and adults with disabilities,
those with substance abuse disorders, and low-income individuals. The types of residents that these providers serve is
shown in Appendix C. According to the Mid-Hudson Regional Community Health Assessment, the top three issues that these
providers felt aected the health in their communities, when considering the Mid-Hudson Region as a whole, were access to
aordable, decent and safe housing; access to mental health providers, and access to aordable, reliable transportation. The
top three barriers that focus group members felt prevented residents from achieving better health in their community were
knowledge of existing resources, health literacy and drug and/or alcohol use.
Also, of note, the additional data sources used to compile the Mid-Hudson Region Community Health Assessment included
the following secondary sources. Monteore St. Luke’s Cornwall used these sources to help support our ndings.
The additional data sources that HealtheConnections utilized to create the overall Mid-Hudson Region Community Health
Assessment included the following:
American Community Survey (ACS): A survey conducted nationally by the U.S. Census Bureau to gather information about
the social and economic need of communities. Secondary source
Behavioral Risk Factor Surveillance System (BRFSS): An annual national phone survey coordinated and funded by the
Centers for Disease Control and Prevention (CDC) and conducted by each State’s health department. Data includes health
related behaviors, health conditions, and use of health services. Secondary source
Comprehensive Housing Aordability Strategy Data (CHAS): Custom tabulations of ACS data about housing problems and
housing needs from the U.S. Census Bureau sent to the U.S. Department of Housing and Urban Development (HUD). HUD and
local governments use this data to plan how to distribute their funds. Secondary source
County Business Patterns: An annual series from the U.S. Census Bureau which provides economic data by industry, such as
number of establishments, employment during a certain week, and annual payroll. Secondary source
County Health Rankings & Roadmaps: A collaboration between the Robert Wood Johnson Foundation and the University
of Wisconsin Population Health Institute. County Health Rankings & Roadmaps pulls from a variety of sources to measure vital
health factors in counties across the U.S.. Secondary source
HRSA Data Warehouse: A website run by the Health Resources and Services Administration (HRSA) which provides maps,
data, reports, and dashboards about HRSA’s health care programs, including health Professional Shortage Areas, Health
Resource Files, and Medically Underserved Populations. Secondary source
Healthy People 2020: A collaborative process that reects input from a diverse group of individuals and organizations.
Healthy People2020 includes 10-year national objectives for improving the health of all Americans. Healthy People has
established benchmarks and monitored progress over time. Secondary source
Map the Meal Gap: A county level analysis of food insecurity conducted by Feeding America using sources, such as the ACS,
the Bureau of Labor Statistics, and the U.S. Department of Agriculture (USDA). Secondary source
Measure of America: A project of the Social Science Research Council that issues reports, briefs, and interactive data
visualizations to provide an understanding of well-being and opportunity in America. Secondary source
National Environmental Public Health Tracking Network: A data hub provided by the CDC which brings together health
and environmental data. Secondary source
New York State Board of Elections: Established as a bipartisan agency of New York State to administer and enforce all laws
relating to elections within the State. Data tracked by the board includes election results and enrollment statistics for New
York State. Secondary source
New York State Communicable Disease Annual Reports: Documents are released annually from NYSDOH containing
mandated reports of suspected or conrmed communicable diseases. Secondary source
New York State Bureau of Sexual Health and Epidemiology: A special projects unit responsible for conducting Sexually
Transmitted Infection (STI) surveillance activities related to screening, disease morbidity, and HIV/STI Partner Services disease
intervention activities. Secondary source
23
New York State Cancer Registry: A registry which collects, processes, and reports information about New Yorkers
diagnosed with cancer from all physicians, dentists, laboratories, and other health care providers, who are required to
report all cancers to the NYSDOH. Secondary source
New York State Department of Health Rabies Laboratory: A system that contains monthly reports of the number of
animals tested for rabies, as well as the number that tested positive for rabies in every New York State county. Secondary
source
New York State Division of Criminal Justice: A criminal justice support agency which provides resources and services
that inform decision-making and improve the quality of the criminal justice system. Secondary source
New York State Education Department (NYSED): NYSED publicly reports educational data submitted by educational
institutions on its website data.nysed.gov. Secondary source
New York State HIV Surveillance System: An HIV surveillance system conducted by the AIDS Institute Bureau of
HIV/AIDS Epidemiology that facilitates and monitors HIV-related laboratory and clinician reporting in New York State.
Secondary source
New York State Hospital-Acquired Infection Program: A program developed to provide data on select hospital-
acquired infections (HAI) that hospitals are required to report by law to the Department of Health. This law was created
to provide the public with fair, accurate, and reliable HAI data to compare hospital infection rates and support quality
improvement and infection prevention activity in hospitals. Secondary source
New York State Immunization Information System: A system that provides a complete, accurate, secure, real-time
immunization medical record that is easily accessible and promotes public health by fully immunizing all individuals
of appropriate age and risk. All health care providers are required to report all immunizations administered to persons
less than 19 years of age, along with the person’s immunization histories, to the New York State Department of Health.
Secondary source
New York Statewide Planning and Research Cooperative System (SPARCS): A comprehensive all-payer data
reporting system established as a result of cooperation between the health care industry and the government. The
system currently collects patient level data on patient characteristics, diagnoses and treatments, services, and charges
for each hospital inpatient and outpatient visit. Secondary source
New York State Department of Transportation: A branch of the New York State government responsible for
administering programs related to the maintenance, coordination, and development of transportation infrastructure.
Secondary source
New York State Student Weight Status Category Reporting System: A system that collects weight status category
data on children and adolescents attending public schools in New York State outside of New York City. Secondary source
Safe Drinking Water Information System: An information hub from the Environmental Protection Agency (EPA)
containing data about public water systems and violations of the EPA’s drinking water regulations, as reported to the EPA
from the states. Secondary source
Small Area Health Insurance Estimates (SAHIE): A program of the U.S. Census Bureau which estimates health
insurance coverage for all states and counties nationally. Secondary source
United for ALICE: Reports which use a standardized methodology that assesses cost of living and nancial hardship on
a county level calculated by United Way of Northern New Jersey. Secondary source
Upstate New York Poison Center: A call center and research organization which provides poison emergency telephone
management, poison information resources, public education, professional education, research and data collection, and
toxicosurveillance in real time. Its coverage area includes all New York State counties except Westchester, New York City,
and Long Island. Secondary source

24
USDA Food Environment Atlas: An atlas from the USDA which assembles data regarding food environment factors, such as
food choices, health and well-being, and community characteristics. Secondary source
Vital Statistics of New York State: A registry of all births, marriages, divorces/dissolutions of marriage, deaths, induced
termination of pregnancy/abortions, and fetal deaths that have occurred in New York State outside of New York City. It is
maintained by the New York State Bureau of Vital Records, a branch of the NYSDOH. Secondary source
The Mid-Hudson Region Community Health Assessment 2019-2021 can be found at the following link:
https://www.orangecountygov.com/180/Community-Health-Assessments--
Secondary Data Collection Plan
Monteore St. Luke’s Cornwall participated in the Orange County Health Summit on June 4, 2019. This summit included
more than 100 community partners including hospitals, health care providers, community members, community health care
providers, and those involved in academia.
This summit was an active working session, to review the data from the above-mentioned Provider focus groups, along with
the Siena College Survey Data and ultimately decide on the Priority Areas for the 2019-2021 Community Health Improvement
and Community Service Plan.
• Arms Acres
• Access: Supports for Living
• Alcohol and Drug Abuse Council of Orange County
• American Heart Association
• American Lung Association
• Action Towards Independence Inc.
• Bon Secours Community Hospital
• Catholic Charities of Orange, Sullivan and Ulster Counties
• Chester Union Free School District
• City of Middletown
• Community advocates
• Cornell Cooperative Extension
• Cornerstone Family Healthcare
• Crystal Run Village Inc.
• Eat Smart New York
• Enlarged Middletown City School District
• Greater Hudson Valley Health System-Orange Regional Medical Center
• Habitat for Humanity of Greater Newburgh
• HealtheConnections
• Honor Emergency Housing Group
• Horizon Family Medical Group
• Hudson River Healthcare
• Hudson Valley Community Services
• Independent Living
• \Keller Army Community Hospital
• Liberty Management
• Maternal Infant Services Network
• Mental Health Association of Orange County
• Monteore St. Luke’s Cornwall Hospital
• NAMI, Orange County NY
25
• Newburgh Seventh Day Adventist Church
• New York State Senator Meztger’s Oce
• Oce for Persons with Developmental Disabilities
• Orange County Oce of Community Development
• Orange County Department of Mental Health
• Orange County Department of Planning
• Orange County Department of Social Services
• Orange County Oce for the Aging
• Orange County Youth Bureau
• Orange-Ulster BOCES
• Planned Parenthood of the Hudson Valley
• RECAP
• Rehabilitation Support Services
• Rockland County Department of Health
• Safe Homes Orange County
• St. Anthony Community Hospital
• SUNY Orange
• Touro College of Osteopathic Medicine
• Tri County Community Partnership
Each participant of the summit was provided with an in-depth overview of the data collected to aid in the selection of the two
priority areas.
The Orange County Department of Health Data Review Guide was provided to all attendees, which outlined the 140 most
current data indicators available, and then compared against the New York State Department of Health Prevention Agenda
Areas specically for Orange County and the state at large. Additionally, a summary of the data collected from the Mid-Hudson
Regional Community Health Survey was presented to all attendees. Furthermore, all summit participants were provided with
data from the Mid-Hudson Region provider survey, which included information from Human Service providers throughout
the region regarding the barriers they saw regarding health for the underrepresented population in the Community Survey
mentioned above. These questions pertained to residents who were among the aging population, veterans, low income,
experiencing homelessness, the LGBTQ community and those with a substance use disorder or mental health diagnosis.
All summit attendees were also given a summary of the prioritization across the Mid-Hudson Region, which utilized the
Hanlon Method. According to the Orange county Department of Health Improvement Plan- the Hanlon Method can be
dened as “a technique created by J.J Hanlon to prioritize health problems. The trusted Hanlon Method minimizes personal bias
and objectively prioritizes health problems based on baseline data and numerical values. This method guides the decision-making
process for selecting health priorities using both the size of the problem and the seriousness of the problem.”
The Orange County Health Summit completed the following tasks:
• In depth review of the most up to date data on all prevention agenda areas
• Provided results from the modied Hanlon Method prioritization
• Full review of the most current community mobilization eorts to best identify the barriers in accessing care in the
City of Newburgh (and MSLC’s Primary Service Area)
• A vote from all participants on the two Prevention Agenda Priorities for the 2019-2021 Community Health
Improvement Plan
• A review of the impacts of the social determinants of health, specically on health outcomes
• Open discussion on assets and barriers of the selected priority areas.

26
Monteore St. Luke’s Cornwall, along with all other Orange County Health Summit participants signed up to participate in
and contribute to strategic planning eorts throughout the course of the 2019-2021 Community Health Improvement Plan.
Of the identied focus areas, each includes a workgroup that is led collaboratively between the Orange County Department
of Health and hospital sta. The purpose of this to ensure that the strategies outlined in the plan are being executed properly.
Each workgroup will report status updates on an annual basis, at what will become a yearly summit.
All of the above was used to create the Orange County Health Improvement Plan 2019-2021, which will support the county-
wide eorts along with participating hospitals (inclusive of Monteore St. Luke’s Cornwall), and specically the 2019-2021
Community Service Plan. The Orange County Health Improvement Plan was distributed to Monteore St. Luke’s Cornwall and
participating community health partners on November 4, 2019 and is available via this link: https://www.orangecountygov.
com/DocumentCenter/View/14537/Orange-County-Community-Health-Improvement-Plan-2019-2021
The rationale behind using this source to help create the Monteore St. Luke’s Cornwall Community Service Plan was that
our eorts moving forward would be best accomplished if we are working in partnership with our fellow community health
partners to create a cohesive approach to tackling the greatest health challenges and priority areas as identied from our
primary and secondary data collection sources.
PRESENTATION OF DATA
Main Health Challenges:
Health Indicators as outlined in the Mid-Hudson Region Community Health Assessment 2019-2021 include Physical Activity,
Nutrition, Mortality, Physical Health including Chronic Diseases such as Chronic Lower Respiratory diseases, asthma,
cardiovascular disease, diabetes, obesity, cirrhosis of the liver, cancer (colorectal, lung and bronchus, prostate, breast, cervical),
Infectious Diseases, Sexually Transmitted Infections, Tick Borne Diseases, Reproductive Health, Oral Health, and Behavioral
Health.
According to the Mid-Hudson Region Community Health Assessment 2019-2021, in Orange County, Heart Disease and cancer
are the leading causes of death and leading causes of premature death (death before age 75) by a large margin. Obesity
is a leading contributor to these top causes of death, as well as diabetes, stroke, and hypertension, all of which can lead to
premature death. According to 2016 BRFSS data, nearly 70% of Orange County adults are either overweight or obese. Data
from 2016-2018 show that 36.8% of school-aged children and adolescents are overweight or obese. Over the past ten years,
the rates of obesity have continually grown, as well as the subsequent morbidity of cardiovascular disease, prediabetes, and
hypertension.
STIs are also on the rise in Orange County. There has been a 75% increase in the average number of newly diagnosed HIV
cases in Orange County from 17.2 per year (2011-2015) to 26.3 per year (2016-2018). Chlamydia rates among both males
and females from 2014-2016 are higher in Orange County than rates in the Mid-Hudson Region, and have steadily increased
or remained the same from 2011-2013 to 2014-2016. Additionally, Orange County had its rst fetal demise in 2019 from
congenital syphilis in over 25 years.
Cardiovascular Disease
While Cardiovascular Disease hospitalization rates have declined across the entire Mid-Hudson Region, from 2007-2014,
Orange County had the highest rate at the time.

27
Orange County had the second highest rate of Age Adjusted Cardiovascular Disease Hospitalization Rate per 10,000 in 2016,
with Sullivan County being the highest.

28
The rate of Cardiovascular Disease in the Hudson Valley is among the highest in Orange County and even higher than the New
York State average. Orange County was also among the highest for Age-Adjusted Cardiovascular Disease Mortality Rates. In
Orange County these rates are above both the Hudson Valley and New York State rates at 223.4 per 100,000 population for
2016.
The hypertension hospitalization rate in Orange County is also higher than the Hudson Valley and New York State rates.
According to the Mid-Hudson Region Community Health Assessment, hypertension is among the risk factors for Cardiovascular
Disease, indicating that Hypertension or high blood pressure occur when the force of blood against the arteries becomes
high enough to cause diseases such as Cardiovascular Disease. Of the 1 in 3 adults in the United States have hypertension and
only about half have it under control. Hypertension can be controlled through checkups with the doctor regularly along with
lifestyle changes.
Orange County had the second highest rate of age-adjusted adults with physician diagnosed hypertension.
While hospitalization rates for hypertension varied across the Mid-Hudson Region, Orange County along with many others
experienced an increase in hypertension related hospitalizations.

29
Orange County was also among the highest for Hypertension related Emergency Department visits
As noted earlier in this report, hypertension was among the top 10 inpatient discharges for Monteore St. Luke’s Cornwall in
2018 and will be included in our focus areas for the 2019-2021 Community Service Plan.
The Mid-Hudson Region Community Health Assessment states that there are three main contributing factors to
Cardiovascular Disease. These factors include: Coronary Heart Disease, Cerebrovascular Disease, otherwise known as Stroke,
and Congestive Heart Failure.
Coronary Heart Disease:
Coronary Heart Disease is the most common type of Cardiovascular Disease and is caused by a buildup of plaque in the
arteries. Orange County had the second highest rate of Coronary Heart Disease hospitalization rates according to the Mid-
Hudson Region Community Health Assessment, with 33.8 per 10,000 in 2016.

30
The complete blockage of arteries may lead to a heart attack. According to the Mid-Hudson Region Community Health
Assessment,
men aged 45 years and older, and women aged 55 years and older, are more likely to have heart attacks
compared to other age groups.
The Mid-Hudson Region Community Health Assessment 2019-2021 states that when stratifying this data by race/ethnicity,
trends are not consistent through each county. For example, non-Hispanic White adults had higher CHD hospitalization
rates compared to the other racial/ethnic groups in Orange, Rockland, and Sullivan Counties. However, in Ulster,
Westchester, New York State, and New York State excluding New York City, non-Hispanic Black adults had higher CHD
Cerebrovascular Disease (Stroke):
The
Mid-Hudson Region Community Health Assessment 2019-2021 states that there are three main types of stroke, ischemic
stroke, hemorrhagic stroke and transient ischemic stroke.
Ischemic stroke occurs when blood clots or plaques block the
blood vessels to the brain, causing the brain to receive decreased oxygen. Almost 87% of strokes are ischemic strokes. A
hemorrhagic stroke occurs when a blood vessel bursts inside the brain, and the blood building up in the tissues causes
severe damage. The signs and symptoms of a stroke must be addressed quickly in order to treat with the best possible
outcomes.
Data from 2016 indicates that Orange County had the highest hospitalization rate of all seven in the mid-Hudson Region.

31
Monteore St. Luke’s Cornwall has put numerous systems into place to address this issue. In April 2006, Monteore St. Luke’s
Cornwall was designated as a New York State Stroke Center and provides high quality, cost eective stroke care to over 300
patients per year. The MSLC Stroke Team is comprised of an interdisciplinary team that utilizes a comprehensive approach
using the American Heart Association/American Stroke Association Guidelines for the Early Management of Acute Ischemic
Stroke.
MSLC is part of the Monteore Health System and has access to the cutting-edge advancements in stroke care through
collaboration with the Moses campus of the Monteore Health System, a designated Joint Commission Certied
Comprehensive Stroke Center and Albert Einstein College of Medicine. Additionally, MSLC has received the American Heart
Association/American Stroke Association’s Get With The Guidelines-Stroke Gold Plus Achievement Award for the tenth
Congestive Heart Failure:
Congestive Heart Failure (CHF) occurs when uid builds up in the lungs, upper or lower extremities or the GI Tract. This causes
the heart to be unable to pump enough blood to meet one’s body’s needs. The Mid-Hudson Region Community Health
Assessment indicates that Orange County was among the highest for CHF hospitalization rates.
The highest rates of CHF hospitalizations in Orange County were among the Non-Hispanic Black population.

32
The Mid-Hudson Region Community Health Assessment 2019-2021 states that obesity was the seventh leading cause of death
in the United States. Diabetes is classied in two forms: Type 1, which is insulin dependent diabetes mellitus, and Type 2, which
is non-insulin dependent diabetes mellitus. Prediabetes is diagnosed when one’s blood sugar level is higher than normal
and is a risk factor of developing diabetes.
According to the NYSDOH, 15-30% of the population in New York State with
prediabetes will develop Type 2 diabetes within ve years, if they do not change their lifestyle behaviors.
According to the Mid-Hudson Region Community Health Assessment 2019-2021, Orange County had the highest percentage of
the population diagnosed with prediabetes, at 12.3%.
Risk factors include obesity/being overweight, genetics, an unhealthy diet, negative health behaviors and decreased
physical activity.
According to the Mid-Hudson Region Community Health Assessment, when stratifying data by race/ethnicity, diabetes
mortality rates were highest among the Non-Hispanic Black population in New York State, as well as New York State
excluding New York City, and most of the counties in the Mid-Hudson Region.

33
Asthma is another key health challenge across the Mid-Hudson region and remains a focus of Monteore St. Luke’s
Cornwall for the last four years. While Orange County was not among the highest percentage of age adjusted adults
with current asthma in 2016, MSLC has partnered with the Orange County Department of Health to address this
challenge specically in the hospital’s Primary Service Area.

34
According to the Mid-Hudson Region Community Health Assessment 2019-2021, Non-Hispanic Black adults had higher rates of
asthma hospitalization compared to Non-Hispanic White and Hispanic Adults.
Of the 65 and older population, Orange County had the second highest rate of Asthma hospitalizations.
Cancer:
The Mid-Hudson Region Community Health Assessment reports that cancer is one of the leading causes of death across all
seven counties in the Mid-Hudson Region. Orange County had the third highest age adjusted all cancer incidence
and mortality rates per 100,000 from 2012-2016.

35
Orange County also had the second highest rate of all cancer incidence and mortality rates, with a higher rate of males in both
incidence and mortality.
Obesity:
The Mid-Hudson Region Community Health Assessment notes that nearly 70% of Orange County adults are overweight or
obese and 26.8% of school-aged children and adults are overweight or obese. Of all seven counties in the region, Orange
County had the highest percentage of adults who are overweight or obese.

36
These rates have been on a steady incline throughout the last ten years, as well as the incidence of morbidity of Cardiovascular
Disease, Prediabetes and Hypertension and will be a key area of focus for MSLC’s 2019-2021 Community Service Plan.
The Mid-Hudson Region Community Health Assessment shows that Sullivan County had the highest rate of obesity among
elementary, middle and high school students when compared to the Mid-Hudson Region, but Orange County rates are still
among the highest in the region.
Sexually Transmitted Infections:
According to the Mid-Hudson Region Community Health Assessment 2019-2021, HIV/AIDS infections continue to be a substantial
public health issue in New York State and the U.S. as a whole. HIV is a preventable disease, and people who are tested and
learn they are HIV-positive can make changes to reduce the risk of transmitting it to their sexual or drug-using partners
signicantly. It is estimated that 91% of new HIV infections in the U.S. are transmitted from people who are not diagnosed or
who are diagnosed, but not in care.
Healthy People 2020 set a target to reduce the number of new HIV diagnoses in the U.S. from 43,806 to 32,855 per year.
Westchester and Sullivan Counties had the highest case rates (10.9 and 10.5), while Putnam had the lowest (1.5). The Mid-
Hudson Region’s rate of newly diagnosed HIV infections was lower than the rate for New York State, which was 16.0 per
100,000 population, including New York City.

37
It is important to note however that here has been a 75%
increase in the average number of newly diagnosed HIV
cases in Orange County from 17.2 per year (2011-2015) to
26.3 per year (2016-2018).
• Orange County’s chlamydia rates stratied by age are
higher than the HV rates and have signicantly worsened
or remained the same from 2011-2013 to 2014-2016
• Chlamydia rates among both males and females from
2014-2016 are higher in Orange County than the HV rates.
Sources: NYSDOH Communicable Disease Electronic
Surveillance System, May 2019 and NYSDOH Community
Health Indicator Reports, 2014-2016
Chlamydia is described as a common STI that infect those of all genders, and while it can be treated easily, if untreated, can
cause major damage to one’s reproductive system. The highest rate of chlamydia in Orange County is among females ages
20-24 years and 15-19 years of age at 2806.8 and 2045.7 per 100,000 population.

38
According to the New York State Department of Health Communicable Disease Electronic Surveillance System, as of May 2019,
the rate of primary and secondary syphilis among females has increased 169% in the last 5 years in New York State.
Orange County had its rst fetal demise from congenital syphilis in over 25 years in 2019.

39
The 2019-2021 Regional Health Assessment Provider Level
Focus Groups also revealed additional issues impacting
Orange County specically include:
Smoking Rates:
• Although overall adult smoking rates decreased from
2013 to 2016—
o The percentage of adult smokers with a
disability is 25.2%
o The percentage of adult smokers with an
income <$25,000 is 26.2%
• Both of these subgroups have smoking rates at nearly
twice the County rate
Source: New York State Department of Health BRFSS 2016-
Orange County Youth Development Survey, 2017.
Access to Supermarkets or a Grocery Store:
• Limited access to supermarkets or other sources of
healthy and aordable food may make it harder to eat a
healthy diet
• Dened as a low-income census tract with at least 500
people, or 33 percent of the population, living more
than 1 mile (urban areas) or more than 10 miles (rural
areas) from the nearest supermarket, supercenter, or
large grocery store
• Orange County has a higher percentage of residents
(4.9%) tting the criteria outlined above than the
Hudson Valley rate and New York State overall.

40
Source: United States Department of Agriculture Food Environment Atlas, 2015
Lead Screenings:
• No safe blood lead level in children has been identied
and lead exposure can aect nearly every system in
the body
• Lead exposure often occurs with no obvious symptoms
and often goes unrecognized
• Two lead screenings by 2 years of age should be part of
routine pediatric care
• Orange County is only testing approximately half of all
children (53.4%) that need to be tested which is worse
than the HV and NYS percentages of 61.6% and 62.8%
respectively
Premature Births:
• Prematurity is the largest contributor to infant
death and leading cause of long-term neurological
disabilities in children
• Overall, County rates are better than in the three cities
• Use real-time birth certicate data to view trends over
time
• Black women in Orange County have the highest
prematurity rates in the County at 11.1%, compared to
all women at 8.1% (2016-2018)
Source: Orange County Birth Certicate Database, as of
February 2019
41
SUMMARY OF KEY FINDINGS:
According to the Mid- Hudson Region Community Health Assessment, Provider Focus Groups, the top-rated issues issue that
aect health in Orange county are the following:
1) Access to aordable, decent, and safe housing
2) Access to aordable, reliable, personal and public transportation
3) Access to mental health providers
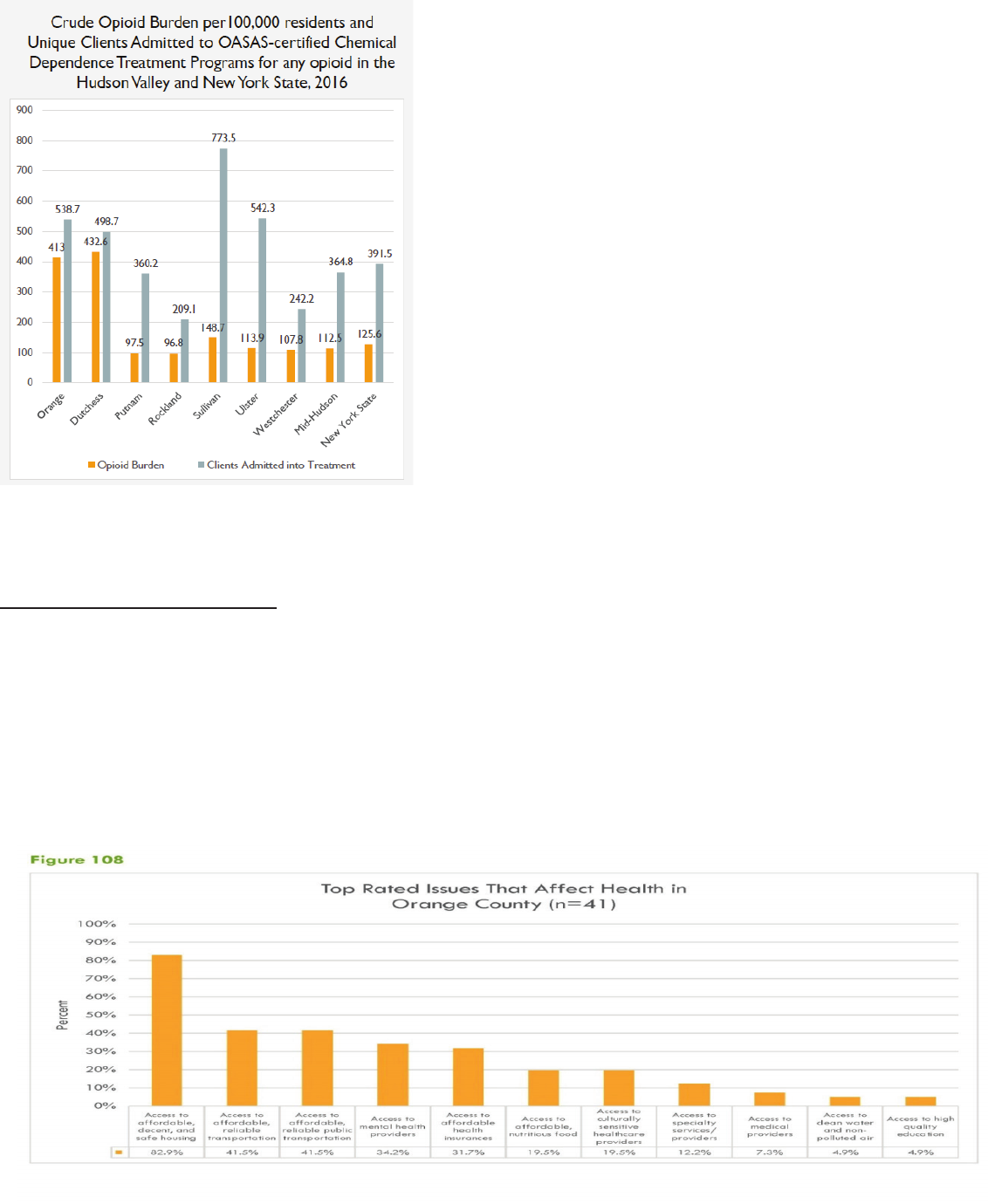
Opioid Burden:
• Opioid burden includes outpatient ED visits and
hospital discharges for non-fatal opioid overdose,
abuse, dependence, and unspecied use; and opioid
overdose deaths
• Orange County has one of the highest burdens
attributed to opioids in the HV
• Overall opioid burden is over 1.5 times the NYS rate
• One of the highest rates in the Hudson Valley for
persons in treatment programs for any opioid use
(including heroin) and just above the NYS rate

42
Safe Housing:
Access to housing was among the top issues identied in the Mid-Hudson Region Community Health Survey across all seven
counties. Of Orange County residents, 14% responded that they were unable to get housing when it was really needed, which
was among the highest of all seven counties (and the same for Dutchess and Westchester).
Transportation:
The vast majority (61%) of Orange County respondents indicated that access to aordable public transportation in their
community was very important.

43
Mental Health:
Of the respondents of the Mid-Hudson Community Health Survey, 52% of residents in Orange County rated their overall
Mental Health as excellent, and 3% rated their mental health as poor.
Furthermore, when asked the question of have you visited a mental health provider in the last 12 months, 51% of Orange
County respondents indicated yes.

44
Additionally, 72% of Orange County residents said they simply chose not to visit a mental health provider
Only 22% of respondents indicated that there are sucient quality mental health providers in Orange County.

45
The New York State Department of Health BRFSS, 2016 Data
indicates that:
• Self-rated health is a commonly used measure of overall well-being
• Survey question asked residents to qualify their mental health: “Thinking
about your mental health, which includes stress, depression, and problems with
emotions, for how many days during the past 30 days was your mental health
not good?”
• Nearly 12% of Orange County residents reported poor mental health 14 or
more days, which is slightly above the HV and NYS percentages.
The top three barriers in achieving beer health in Orange county include:
1) Knowledge of existing resources
2) Drug and/or alcohol use
3) Healthy literacy
The overall impact of health issues in Orange County include the following:
• Chronic Disease (heart disease, diabetes, asthma, obesity, etc.)
• Health disparities
• Mental Health and Substance Abuse Issues
• Maternal and Child Health Issues
• Environmental Factors (built environment, air/water quality, injuries, etc.)
• Prevent communicable diseases (sexually transmitted infections, Hepatitis C, HIV, vaccine preventable diseases,
hospital acquired infections, etc.)
46
In Orange County, the leading causes of death and premature death (before age 75) are heart disease and cancer, with obesity
being the leading contributor to these top causes.
Orange County also has worse than New York State averages (or getting worse since the last assessment) in the following
health areas:
• Overdose deaths due to opioid and heroin use
• Premature births among Non-Hispanic Black women and Hispanic women
• Preventable adult hospitalizations
• Youth-reported alcohol and electronic vaping product use
• Unintended pregnancy among Non-Hispanic Black women and Hispanic women
Emerging issues also include:
• Sexually Transmitted Infections including chlamydia, syphilis, and HIV
• Opioid burden, including hospitalizations, overdoses and deaths
• Youth reported electronic vaping product use
• Prediabetes among adults.
As mentioned above, the Orange County Department of Health participated in the Mid-Hudson Regional Community Health
Survey to collect data on 850 residents to best understand the needs of the community. Key ndings of this survey include:
• 81% of Orange County respondents (93% of respondents with <$25K yearly income), reported that accessible and
convenient transportation was very important or somewhat important to them
• 80% of Orange County respondents (91% of respondents with <$25K yearly income), reported that people may have a
hard time nding a quality place to live due to the high cost of living
• 39% of Orange County respondents living in rural areas reported that places in Orange County did not feel safe vs.
54% of Orange County respondents living in urban zip codes
• 27% of Orange County respondents with <$25K yearly income reported experiencing a mental health condition or
substance or alcohol use disorder compared to 14% of total Orange County respondents
• 28% of Orange County respondents with <$25K yearly income reported that in the past 12 months, they or any other
member of their household has been unable to get food compared to 11% of total Orange County respondents
• 35% of Orange County respondents with <$25K yearly income reported that in the past 12 months, they or any other
member of their household has been unable to get medicine In addition to what was revealed in the Mid-Hudson
Community Health Survey the Provider Focus Group’s also indicated that the Top three issues that impact health in
Orange County were:
Special considerations include that a further drill down of the data is not yet available. The overall results of the assessment
mask some of the disparities that exist in the urban and rural communities within Orange County and specically the City of
Newburgh. SUNY Albany has partnered with the Orange County Department of Health to provide zip code level data based
on the ndings of the community health surveys, but this breakdown will not be available until March of 2020. This has
created a barrier in MSLC’s ability to further analyze the results specic to the hospital’s Primary Service Area. MSLC has been
in discussion with the Orange County Department of Health to discuss specic areas of concern and focus for the 2019-2021
Community Health Improvement plan, specically relating to the high rates of Chlamydia, Syphilis and Gonorrhea in Orange
county in 2018. Additionally, food security is a severe issue in MSLC’s Primary Service area, with only 12% of residents indicat-
ing that they are able to access aordable food that is healthy and nutritious. These will be key areas of focus in MSLC’s Com-
munity Service Plan Workplan.
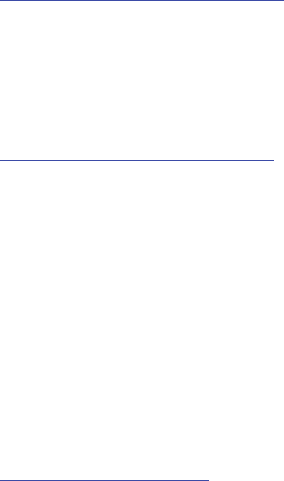
47
Implementation Strategy Report:
The New York State Prevention Agenda Health Improvement Plan for 2019 established ve Prevention Agenda Priority areas:
• Prevent chronic diseases
• Promote a healthy and safe environment
• Promote healthy women, infants and children
• Promote well-being and prevent mental substance use disorders
• Prevent communicable diseases
The Orange County Department of Health has selected the following two priority areas, and as a result of the collaboration
that exists between the Orange County Department of Health, Monteore St. Luke’s Cornwall and several other community
partners, MSLC has also selected the same Priority Areas.
1. Prevent Chronic Disease
2. Prevent Communicable Disease
Service Area for Community Health Assessment and Community Health Improvement Plan:
Orange County
Participating Local Health Department: Orange County Department of Health
Participating Hospitals: Bon Secours Community Hospital, Monteore St. Luke’s Hospital, Orange Regional Medical Center,
and St. Anthony Community Hospital
Orange County Department of Health:
Jackie Lawler, Epidemiologist
845.615.3884
jlawler@orangecountygov.com
Bon Secours Community Hospital and St. Anthony Community Hospital:
Barbara Demundo, System Director, Community Engagement
845.368.5545
Monteore St. Luke’s Cornwall:
Kate Dabroski, Vice President, Marketing, Public and Community Relations
845.784.3850
kdabroski@monteoreslc.org
Orange Regional Medical Center:
Amanda Langseder, Director of Community Health
845.794.3300 ext. 2187
alangseder@ghvhs.org
The signicant needs to be addressed by Monteore St. Luke’s Cornwall, focusing on Orange County and specically the
hospital’s Primary Service Area inclusive of the City of Newburgh are broken down in the following:

48
Prevent Chronic Disease: Monteore St. Luke’s Cornwall will focus on preventative care and management with an eort to
promote evidenced based care to prevent and manage chronic diseases including Cardiovascular Disease, COPD, Diabetes
and Prediabetes as well as Asthma. The MSLC team already has many systems in place to address these areas. Additionally,
MSLC will work to increase food security in Orange County by improving screening methods to identify patients with food
insecurity, and further enhance the resources available within the hospital and amongst our community partners to connect
the populations we serve with more available healthier food sources. Another focus area will be increasing cancer screening
rates.
Prevent Communicable Disease: Monteore St. Luke’s Cornwall will be working with community partners to reduce the
annual rate of growth for Sexually Transmitted Infections. There has been a signicant increase in STIs in Orange county and
MSLC has seen this increase rst hand in both the presentations to the Emergency Department as well as the Labor and
Delivery Unit.
Signicant Needs Not Addressed:
Promote Healthy Women Infants and Children:
o The City of Newburgh also has higher than Orange County average rates for premature births, 10.5% as
compared to the goal of 8.4% and a baseline of 9.5% from 2013-2015.
o The rates of teen pregnancy in Newburgh are twice the County average at 53.7 per 1,000 families.
Alternate Resources: Monteore St. Luke’s Cornwall has put into place several initiatives in its Birthing
Center to work with patients from the beginning of their pregnancy and post-partum.
Explanation of Rationale: While this is not a priority area of Monteore St. Luke’s Cornwall for the 2019-2021
Community Service Plan, many systems are already in place in this regard.
• In 2018, an OB Patient Navigator was added to the MSLC Birthing Center Sta. Local OB oces in the community
provide MSLC with patient lists of those due three to four months ahead of presentation to hospital. The
Navigator makes outreach to these patients and oers tours of the facility.
• In addition, prenatal education and breastfeeding classes are oered and the course size has increased from one
to three couples to approximately 10 couples per course in 2018.
• In 2019, a Patient Navigator was hired to connect patients who struggle with substance abuse or opioid
addiction with the appropriate community resources. This position is grant funded through the Dyson
Foundation through September 2020.
Promote a Healthy and Safe Environment:
Access to Supermarket or Grocery Stores:
• Limited access to supermarkets or other sources of healthy and aordable food may make it harder to eat a
healthy diet
• Dened as a low-income census tract with at least 500 people, or 33 percent of the population, living more
than 1 mile (urban areas) or more than 10 miles (rural areas) from the nearest supermarket, supercenter, or large
grocery store
• Orange County has a higher percentage of residents tting the criteria outlined above than the Hudson Valley
Rate and NYS overall
Explanation of Rationale: Monteore St. Luke’s Cornwall is indirectly addressing this in the realm of working to increase
food security in the community we serve. By working with the community to enhance the availability of healthy food
options, this may ultimately impact this disparity.

49
Lead Screenings:
• No safe blood lead level in children has been identied and lead exposure can aect nearly every system in the
body
• Lead exposure often occurs with no obvious symptoms and often goes unrecognized
• Two lead screenings by 2 years of age should be part of routine pediatric care
• Orange County is only testing approximately half of all children (53.4%) that need to be tested which is worse
than the HV and NYS percentages of 61.6% and 62.8% respectively
Explanation of Rationale: This is not an area of focus at Monteore St. Luke’s Cornwall however community-based
pediatricians perform lead screenings in MSLC’s Primary Service Area.
Promote well-being and prevent mental substance use disorders
• Orange county has one of the highest burdens attributed to opioids in the Hudson Valley. Orange county also
has one of the highest rates in the Hudson Valley for persons in treatment programs for any opioid use including
heroin and is just above the NYS State Average.
Explanation of Rationale: While this may not be addressed in MSLC’s three-year Community Health Improvement/
Community Service Plan, this remains a top focus throughout the hospital and Orange county as a whole. At the June
4, 2019 Community Health Summit, Orange County Commissioner of Mental Health, Darcie Miller stated that there
are already a large variety of resources invested in addressing the opioid epidemic and our collective eorts for the
identication of Priority areas and Community Service Plan would be best geared in other directions. Additionally,
In 2019, MSLC launched the rst Medication Assisted Treatment Program, within the walls of the hospital, engaging
patients when they rst arrive and working to get them connected to the proper community resources.
Thank you for allowing us the opportunity to share the Health Needs Assessment of the Mid-Hudson Region of New York, and
specically the Community that Monteore St. Luke’s Cornwall is proud to serve.

List of Appendices 323
APPENDIX A
REGIONAL COMMUNITY HEALTH ASSESSMENT SURVEY
Hello, this is _____ for the Siena College Research Institute. We are working with local health departments and hospital
systems to survey Hudson Valley residents to better understand the health status and health-related values of people
who live in the community.
IF NEEDED:
You’ve been selected at random to be included in this survey. Your individual responses are confidential and no
identifiable information about you will be shared with anyone—all responses are grouped together. The questions I am
going to ask you to relate to your health and to your thoughts about health-related resources in your community. Again,
your responses may really help to strengthen health policies and services.
IF NEEDED:
In total, the survey takes approximately ____ minutes to complete and you may refuse to answer any question that you
do not want to answer. Are you able to help us with this important project? (NOW IS ALSO A TIME TO OFFER A CALL
BACK AT A SPECIFIC, REQUESTED TIME AND PHONE NUMBER)
1. Overall, would you say that the quality of life in your community is excellent, good, fair or poor?
A. Excellent
B. Good
C. Fair
D. Poor
2. What State do you live in? [If not NY or CT, terminate]
3. What County do you live in? [If not Dutchess, Orange, Rockland, Putnam, Sullivan, Ulster Westchester or Litchfield CT
(?), terminate]
4. What is your zip code? _____________
5. How long have you lived in _______ County?
a. Less than 1 year
b. 1-5 years
c. More than 5 years
6. I’m going to read you a series of statements that some people make about the area around where they live, that is,
their community. For each, tell me if that statement is completely true of your community, somewhat true, not very true
or not at all true for your community.
A. There are enough jobs that pay a living wage.
B. Most people are able to access affordable food that is healthy and nutritious.
C. People may have a hard time finding a quality place to live due to the high cost of housing.
D. Parents struggle to find affordable, high-quality childcare.
E. There are sufficient, quality mental health providers.
F. Local government and/or local health departments, do a good job keeping citizens aware of potential public health
threats.
G. There are places in this community where people just don’t feel safe.
H. People can get to where they need using public transportation.
List of Appendices 324
7. How important is it to you that the community where you live have the following?
A. Accessible and convenient public transportation
B. Affordable public transportation
C. Well-maintained public transportation vehicles
D. Safe public transportation stops or waiting areas
E. Special transportation services for people with disabilities or older adults
8. Overall, how would you rate the community you live in as a place for people to live as they age?
A. Excellent
B. Good
C. Fair
D. Poor
E. I don’t know
9. For each of the following aspect of life, please rate it as excellent, good, fair, or poor in your community. Please let me
know if you simply do not know enough to say.
A. The availability of social/civic programs for seniors
B. The quality of health care services for seniors
C. The availability of programs and activities for youth outside school hours
D. The quality of information from county agencies during public emergencies, such as weather events or disease
outbreaks
10. In general, how would you rate your health? Would you say that your health is excellent, good, fair or poor?
A. Excellent
B. Good
C. Fair
D. Poor
11. Have you ever been told by a doctor or other health professional that you have any chronic health condition, such as
high blood pressure, diabetes, high cholesterol, asthma or arthritis?
A. Yes
B. No
12. If YES to 11--How confident are you that you can manage your physical health condition?
A. Very Confident
B. Somewhat Confident
C. Not Very Confident
D. Not at all confident
13. Mental health involves emotional, psychological and social wellbeing. How would you rate your overall mental
health? Would you say that your mental health is excellent, good, fair or poor?
AS NEEDED: This includes things like hopefulness, level of anxiety and depression.
A. Excellent
B. Good
C. Fair
D. Poor
14. Have you ever experienced a mental health condition or substance or alcohol use disorder?
A. Yes
List of Appendices 325
B. No
15. If YES to 14--How confident are you that you can manage your mental health condition?
A. Very Confident
B. Somewhat Confident
C. Not Very Confident
D. Not at all confident
16. Thinking back over the past 12 months, for each of the following statements I read, tell me how many days in an
AVERAGE WEEK you did each. Over the past 12 months how many days in an average week did you… (responses are 0
days, 1-3 days, 4-6 days or all 7 days)
A. Ate a balanced, healthy diet
B. Exercised for 30 minutes or more a day
C. Got 7-9 hours of sleep in a night
17. On an average day, how stressed do you feel?
AS NEEDED: Stress is when someone feels tense, nervous, anxious, or can’t sleep at night because their mind is troubled.
A. Not at all stressed
B. Not very stressed
C. Somewhat stressed
D. Very stressed
18. In your everyday life, how often do you feel that you have quality encounters with friends, family, and neighbors that
make you feel that people care about you? (IF NEEDED: For example, talking to friends on the phone, visiting friends or
family, going to church or club meetings)
A. Less than once a week
B. 1-2 times a week
C. 3-5 times a week
D. More than 5 times a week
19. Have you smoked at least 100 cigarettes in your entire life?
A. Yes
B. No
20. If YES to 19, do you now smoke cigarettes every day, some days, or not at all?
A. Everyday
B. Some days
C. Not at all
21. Pertaining to alcohol consumption, one drink is equivalent to a 12-ounce beer, a 5-ounce glass of wine, or a drink
with one shot of liquor. During the last 30 days, on the days when you drank, about how many drinks did you drink on
average? [If respondent gives a range, ask for one whole number. Their best estimate is fine. If they do not drink, enter
0.]
_______ drinks
22. [If Q21>0] Considering all types of alcoholic beverages, how many times during the past 30 days did you have X [5 for
men, 4 for women] or more drinks on an occasion?
A. _____ number of times
B. None
List of Appendices 326
23. How frequently in the past year have you used an illegal drug or used a prescription medication for non-medical
reasons?
A. Never
B. Less than once per month
C. More than once per month, but less than weekly
D. More than once per week, but less than daily
E. Daily
24. In the past 12 months, have you or any other member of your household been unable to get any of the following
when it was really needed? Please answer yes or no for each item.
A. Food
B. Utilities, including heat and electric
C. Medicine
D. Any health care, including dental or vision
E. Phone
F. Transportation
G. Housing
H. Childcare
25. Have you visited a primary care physician for a routine physical or checkup within the last 12 months?
A. Yes
B. No
26. If NO to question 25, in the last 12 months, were any of the following reasons that you did not visit a primary care
provider for a routine physical or checkup? (SELECT ALL THAT APPLY)
A. I did not have insurance
B. I did not have enough money (prompt if needed: for things like co-payments, medications, etc)
C. I did not have transportation
D. I did not have time
E. I chose not to go
F. Other_________________________________
27. Have you visited a dentist for a routine check-up or cleaning within the last 12 months?
A. Yes
B. No
If NO to question 27, in the last 12 months, were any of the following reasons that you did not visit a dentist for a
routine check-up or cleaning? (SELECT ALL THAT APPLY)
A. I did not have insurance
B. I did not have enough money (prompt if needed: for things like co-payments, medications, etc)
C. I did not have transportation
D. I did not have time
E. I chose not to go
F. Other_________________________________
Sometimes people visit the emergency room for medical conditions or illnesses that are not emergencies; that is, for
health-related issues that may be treatable in a doctor’s office.
28. Have you visited an emergency room for a medical issue that was not an emergency in the last 12 months?
A. Yes
List of Appendices 327
B. No
29. If YES to question 28, in the last 12 months, for which of the following reasons did you visit the emergency room for
a non-health emergency rather than a doctor’s office? (SELECT THE BEST (1) OPTION)
A. I do not have a regular doctor/primary care doctor
B. The emergency room was more convenient because of the location
C. The emergency room was more convenient because of the cost
D. The emergency room was more convenient because of the hours of operation
E. At the time I thought it was a health-related emergency, though I later learned it was NOT an emergency
If yes to 13 (behavioral health condition)
30. Have you visited a mental health provider, such as a psychiatrist, psychologist, social worker, therapist for 1-on-1
appointments or group-sessions, etc. within the last 12 months?
A. Yes
B. No
31. If NO to question 30, in the last 12 months, were any of the following reasons that you did not visit a mental health
provider? (SELECT ALL THAT APPLY)
A. I did not have insurance
B. I did not have enough money (prompt if needed: for things like co-payments, medications, etc)
C. I did not have transportation
D. I did not have time
E. I chose not to go
F. Other_________________________________
32. How likely would you be to participate in the following types of programs aimed at improving your health? Would
you be very likely, somewhat likely, not very likely or not at all likely?
A. A mobile app based program on your smart phone
B. An in person, one-on-one program
C. An in person, group program
D. An online, computer based, one-on-one program
E. An online, computer based, group program
We are just about finished. These last few questions are about you.
33. Are you Hispanic?
A. Yes
B. No
34. What is your race?
A. White
B. Black
C. Asian
D. Other
35. Do you have health insurance?
a. Yes
b. No
List of Appendices 328
36. What is your source of health insurance?
a. Employer
b. Spouse/Partner’s employer
c. NYS Health Insurance marketplace/Obamacare
d. Medicaid
e. Medicare
f. None
g. Other
37. What is your living arrangement? Do you…
A. Rent an apartment or home
B. Own your own
C. Other living arrangement
38. What is your employment status?
A. Employed full time
B. Employed part-time
C. Unemployed, looking for work
D. Unemployed, not looking for work
E. Retired
39. Are there children <18 living in your household?
A. Yes
B. No
40. Are you or anyone in your household a veteran or a member of active duty military service?
A. Yes
B. No
41. Do you or anyone in your household have a disability?
A. Yes
B. No
42. About how much is your total household income, before any taxes? Include your own income, as well as your spouse
or partner, or any other income you may receive, such as through government benefit programs. (READ THE
FOLLOWING OPTIONS)
A. Less than $25,000
B. $25,000 to $49,999
C. $50,000 to $99,999
D. $100,000 to $149,999
E. $150,000 or more
43. What is your gender?
A. Male
B. Female
C. Transgender/other gender

List of Appendices 329
APPENDIX B
Stakeholder Interview Form
1. Name_________________________________________________
2. Organization ___________________________________________
3. Organization Website ____________________________________
4. Position_______________________________________________
5. What is your service area?
On website
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
6. Who do you serve? Please check all that apply
Infants and toddlers
Children
Adolescents
Adults
Seniors
Veterans
English as a second language
Women (services specifically for women)
Men (services specifically for men)
LGBTQ
Those with a substance use disorder
Those with a mental health diagnosis
People with disabilities
People experiencing homelessness
Incarcerated or recently incarcerated
Low income
General population
All the above
7. Thinking about the populations that you serve, what are the top 3 issues that affect health in the communities
you serve?
Access to affordable nutritious food
Access to affordable, decent and safe housing
Access to affordable, reliable transportation
Access to affordable, reliable public transportation
Access to culturally sensitive health care providers
Access to affordable health insurances
Access to clean water and non-polluted air
Access to medical providers
Access to mental health providers
Access to high quality education
Access to specialty services/providers
List of Appendices 330
8. Which of the following are the top 3 barriers to people achieving better health in the communities you serve?
Knowledge of existing resources
Geographic location – living in an urban area
Geographic location – living in a rural area
Health literacy
Having someone help them understand insurance
Having someone to help them understand their medical condition
Having a safe place to play and/or exercise
Quality of education
Attainment of education
Drug and/or alcohol use
Cultural Customs
Other (specify) __________________
9. Besides lack of money, what are the underlying factors and barriers to solving the top 3 issues you identified
in the communities you serve?
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
10. What evidence-based interventions (if any) do you use that target your populations to address the social
determinants of health?
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
List of Appendices 331
11. As we go through the following list of health issues, please rate from 1 to 5 the impact of the health issues in
your service area with 1 being very little and 5 being highly impacted.
Chronic Disease (e.g. heart disease, diabetes, asthma, obesity, cancer, etc.)
(Very Little) 1 2 3 4 5 (Highly Impacted)
Health Disparities
(Very Little) 1 2 3 4 5 (Highly Impacted)
Mental Health and Substance Use Issues
(Very Little) 1 2 3 4 5 (Highly Impacted)
Maternal and Child Health issues
(Very Little) 1 2 3 4 5 (Highly Impacted)
Environmental Factors (e.g. built environment, air/water quality, injuries, falls, food safety)
(Very Little) 1 2 3 4 5 (Highly Impacted)
Prevent Communicable diseases (e.g. sexually transmitted infections, hepatitis C, HIV, vaccine
preventable disease, hospital acquired infections, etc.)
(Very Little) 1 2 3 4 5 (Highly Impacted)
