
Security-
Widefield
El Paso County | Colorado
INFORMATION TO PROTECT OUR COMMUNITIES
Per- and Polyfluoroalkyl
Substances (PFAS)
Exposure Assessment
REPORT
6/14/22
i
Table of Contents
Abbreviations .................................................................................................... iii
Executive Summary ....................................................................................... ES-1
Background and Purpose ........................................................................................................... ES-1
Exposure Assessment Activities ................................................................................................. ES-2
Security-Widefield Community-Wide Findings ............................................................................ ES-3
Limitations ................................................................................................................................ ES-6
Recommendations .................................................................................................................... ES-6
For More Information ................................................................................................................ ES-8
Background and Purpose .................................................................................... 1
What Are PFAS? ............................................................................................................................. 1
Why Security-Widefield? ................................................................................................................ 3
Methods ............................................................................................................. 4
Sampling Frame .............................................................................................................................. 4
Participant Eligibility ....................................................................................................................... 6
Participant Recruitment.................................................................................................................. 6
Data Collection and Analysis ........................................................................................................... 6
Results .............................................................................................................. 13
Profile of Security-Widefield (El Paso County) EA Participants ........................................................ 13
Comparison of Security-Widefield EA Participants’ Demographics to Sampling Frame
Demographics .............................................................................................................................. 15
PFAS in Blood ............................................................................................................................... 16
PFAS in Urine ............................................................................................................................... 34
PFAS in Tap Water ........................................................................................................................ 35
PFAS in Household Dust ................................................................................................................ 36
Discussion ......................................................................................................... 38
Generalizability of Security-Widefield EA Community Statistics ..................................................... 39
Relationships Between Demographics and PFAS Blood Levels ........................................................ 39
Significance of Drinking Water Exposures ...................................................................................... 40
Other Exposure Characteristics ..................................................................................................... 42
Security-Widefield Community-Wide Findings .................................................. 42
Limitations ................................................................................................................................... 45
Recommendations ....................................................................................................................... 46
For More Information ................................................................................................................... 47
References ........................................................................................................ 48
Appendix A: Additional Tables
Appendix B: Additional Background Statistics
Appendix C: PFAS Blood Levels by Demographics and Exposure Characteristics

ii
Tables
Table 1. Summary of recruitment and data collection efforts ..................................................................... 9
Table 2. List of PFAS measured for in blood, urine, tap water, and dust ................................................... 10
Table 3. Characteristics of Security-Widefield EA participants ................................................................... 14
Table 4. Demographic comparison of EA participants and the sampling frame population ...................... 16
Table 5. Community statistics for PFAS in blood in micrograms per liter .................................................. 17
Table 6. Geometric means for PFAS in blood in micrograms per liter, unadjusted and age-adjusted to
the sampling frame ..................................................................................................................................... 18
Table 7. Comparison of PFAS blood geometric means (GMs) and 95th percentiles in Security-
Widefield, Colorado, with the U.S. population (NHANES 2015–2016) in micrograms per liter ................. 20
Table 8. Pearson correlation coefficients between PFAS in blood (log) ..................................................... 21
Table 9. Summary of statistically significant variables (p<0.05) in multivariate regression models .......... 23
Table 10. Community statistics for PFAS in urine reported in micrograms per liter .................................. 35
Table 11. Summary statistics for dust samples (n=18) collected in Security-Widefield ............................. 36
Figures
Figure 1. Sampling frame for the Security-Widefield Exposure Assessment ................................................ 5
Figure 2. Distribution of PFAS blood levels (log scale) ................................................................................ 18
Figure 3. EA average PFAS blood levels compared to national levels ........................................................ 21
Figure 4. PFAS blood levels in adults and children (log scale) .................................................................... 25
Figure 5. PFAS blood level in adults by sex (log scale) ................................................................................ 26
Figure 6. PFAS blood level in adults by drinking water source (log scale) .................................................. 27
Figure 7. PFAS blood level in adults by filter type (log scale) ..................................................................... 28
Figure 8. PFAS blood level in adults by tap water consumption rates (log scale) ...................................... 29
Figure 9. PFAS blood levels in adults by length of residence in sampling frame (log scale) ....................... 30
Figure 10. PFAS blood level in adults by public water supply (log scale) .................................................... 31
Figure 11. PFAS blood level in adults by occupational history (log scale) .................................................. 32
About ATSDR
The Agency for Toxic Substances and Disease Registry (ATSDR) is a federal
public health agency of the U.S. Department of Health and Human Services
(HHS). ATSDR works with other agencies and state, tribal and local
governments to protect communities from harmful health effects related
to exposure to natural and manmade hazardous substances. For more
information about ATSDR, visit https://www.atsdr.cdc.gov/
.

iii
Abbreviations
9Cl-PF3ONS 9-chlorohexadecafluoro-3-oxanone-1-sulfonic acid
11Cl-PF3OUdS 11-chloroeicosafluoro-3-oxaundecane-1-sulfonic acid
AFCEC Air Force Civil Engineer Center
AFFF aqueous film forming foam, also known as “A triple F”
ATSDR Agency for Toxic Substances and Disease Registry
CDC Centers for Disease Control and Prevention
DONA 4,8-dioxa-3H-perfluorononanoic acid
EA exposure assessment
EPA U.S. Environmental Protection Agency
EtFOSAA N-ethyl perfluorooctanesulfonamidoacetic acid
FOD frequency of detection
FtS 4:2 fluorotelomer sulfonic acid 4:2
FtS 6:2 fluorotelomer sulfonic acid 6:2
FtS 8:2 fluorotelomer sulfonic acid 8:2
GAC granular activated carbon
HA health advisory
HFPO-DA (GenX) hexafluoropropylene oxide dimer acid
LOD limit of detection
MeFOSAA N-methyl perfluorooctanesulfonamidoacetic acid
MHP mobile home park
µg/L, or ug/L micrograms per liter (same as parts per billion or 1,000 parts per trillion)
ng/g nanograms per gram (same as parts per billion or micrograms per kilogram)
NHANES National Health and Nutrition Examination Survey
N-EtFOSA N-ethyl perfluorooctanesulfonamide
N-EtFOSE N-ethyl perfluorooctanesulfonamidoethanol
N-MeFOSA N-methyl perfluorooctanesulfonamide
N-MeFOSE N-methyl perfluorooctanesulfonamidoethanol
n-PFOA linear isomer of PFOA
n-PFOS linear isomer of PFOS
PFAS per- and polyfluoroalkyl substances
PFAS-AWARE PFAS Assessment of Water and Resident Exposure
PFBA perfluorobutanoic acid
PFBS perfluorobutane sulfonic acid
PFDA perfluorodecanoic acid
PFDoA perfluorododecanoic acid
PFDS perfluorodecane sulfonic acid
PFDoS perfluorododecanesulfonate
PFHpA perfluoroheptanoic acid
PFHpS perfluoroheptane sulfonic acid
PFHxA perfluorohexanoic acid

iv
PFHxS perfluorohexane sulfonic acid
PFNA perfluorononanoic acid
PFNS perfluorononane sulfonic acid
PFOA perfluorooctanoic acid
PFOS perfluorooctane sulfonic acid
PFOSA perfluorooctanesulfonamide
PFPeA perfluoropentanoic acid
PFPeS perfluoropentane sulfonic acid
PFTA perfluorotetradecanoic acid
PFTrA perfluorotridecanoic acid
PFUnA perfluoroundecanoic acid
ppt parts per trillion (same as 1 nanogram per liter)
Sb-PFOA branched isomers of PFOA
Sm-PFOS branched isomers of PFOS
WD water district
WSD water and sanitation district
ES-1
Executive Summary
Background and Purpose
PFAS (or per- and polyfluoroalkyl substances) are a family of synthetic chemicals that have been used in
industry and consumer products since the 1950s. There are thousands of different PFAS. This
assessment discusses some of the most commonly studied PFAS, including perfluorooctanoic acid
(PFOA), perfluorooctane sulfonic acid (PFOS), perfluorohexane sulfonic acid (PFHxS), perfluorononanoic
acid (PFNA), perfluorodecanoic acid (PFDA), perfluoroundecanoic acid (PFUnA), and N-methyl
perfluorooctanesulfonamidoacetic acid (MeFOSAA).
PFAS do not occur naturally but are widespread in the environment. They have been found in soil,
water, air, and animal and plant life. Most PFAS (including PFOA, PFOS, PFHxS, and PFNA) are either very
resistant to breaking down or degrade into other PFAS that do not degrade further. Major exposure
routes for PFAS include drinking contaminated water and eating contaminated food, but exposure can
also occur through other routes (i.e., ingestion of contaminated dust). Once PFAS enter people’s bodies,
some of them (including PFOA, PFOS, PFHxS, and PFNA) can remain in the body for long periods and can
be measured in the blood years after exposure. Most people in the United States have been exposed to
PFAS. At least one PFAS was detected in more than 99% of National Health and Nutrition Examination
Survey (NHANES) samples collected for the 1999-2000 survey cycle.
The Centers for Disease Control and Prevention (CDC) and the Agency for Toxic Substances and Disease
Registry (ATSDR) are conducting exposure assessments (EAs) in communities that were known to have
PFAS in their drinking water and are near current or former military bases. This report shares results
from the community of Security-Widefield in El Paso County, Colorado, near Peterson Air Force Base
(the Base). When all EAs are complete, ATSDR will prepare a report describing the results across all sites.
Possibly as early as the 1970s, the Base used aqueous film forming foam (AFFF) containing PFAS for its
firefighter training. Over time, the PFAS from the AFFF entered the ground, moved into the groundwater
to offsite locations, and affected nearby municipal wells. PFAS were first detected in municipal wells
downgradient of the Base in 2013. The affected wells supplied water to customers from the Security
Water District (WD), the western portion of the Widefield Water and Sanitation District (WSD), and the
Security Mobile Home Park (MHP). Between January and November of 2016, Security WD and Widefield
WSD inactivated their contaminated groundwater wells and shifted to uncontaminated surface water
sources. In 2017, Widefield WSD installed an ion exchange system to treat PFAS in water from its
contaminated wells. Security WSD currently uses uncontaminated surface water sources. Residents of
Security MHP were provided bottled water beginning in the summer of 2016 until a treatment system
was installed in November of 2017. From 2018 to 2019, a PFAS Assessment of Water and Resident
Exposure (PFAS AWARE) study was conducted by the Colorado School of Public Health and the Colorado
School of Mines that evaluated exposure to PFAS in drinking water in the El Paso County community.
The PFAS AWARE study evaluated 200 participants in 2018 and resampled 50 of the participants in 2019.
The study evaluated serum PFAS along with markers of health related to liver function, cholesterol, and
immune response. The results of the study indicated that the primary source of PFAS in people’s blood
was PFAS in the drinking water.
Based on the information ATSDR has reviewed, the public drinking water supplies in Security-Widefield
currently meet or are below the U.S. Environmental Protection Agency’s (EPA) 2016 health advisory
(HA). At this time, ATSDR does not recommend community members who get drinking water from
Security WD, Widefield WSD, or Security MHP use alternative sources of water.

ES-2
This EA assessed PFAS levels in the blood and urine of Security-Widefield residents. Test results were
compared to PFAS levels in a nationally representative sample. Tap water and indoor dust samples from
a subset of households were analyzed. These EA results will help participants and their communities
better understand their PFAS exposure, allow ATSDR to provide recommendations to reduce exposure,
and inform public health efforts related to protecting communities from sources of PFAS other than
contaminated drinking water supplies.
ATSDR will use the data collected from this and other EAs to help inform future studies of PFAS
exposure.
Exposure Assessment Activities
ATSDR invited a randomly selected sample of Security-Widefield households to participate in this EA. To
be eligible to participate, household residents must have (1) been served by the drinking water systems
of Security Water District (WD), Security Mobile Home Park (MHP), or the western portion of the
Widefield Water and Sanitation District (WSD) for at least 1 year before November 10, 2016 (these
residents have the greatest likelihood of past exposures to PFAS via drinking water), (2) been greater
than three years old at the time of sample collection, and (3) not been anemic or had a bleeding
disorder that would prevent giving a blood sample. Results from randomly selected households allow
ATSDR to estimate exposure for all community members, even those who were not tested.
In September 2020, 346 eligible people (318 adults and 28 children) from 188 households participated in
the EA sample collection event. ATSDR performed the following tasks:
• administered exposure history questionnaires to all participants
• collected blood and urine samples from every participant
• collected tap water and dust samples from the homes of 18 randomly selected participants
• tested for 7 PFAS in blood, 14 in urine, 18 in water, and 33 in dust
1
• measured PFHxS, PFOS, PFOA, PFNA, PFDA, and PFUnA across all media (blood, urine, tap water,
and dust)
• mailed individual biological and environmental results to participants in May 2021
This report summarizes community PFAS blood levels, measured in serum, for the group of Security-
Widefield residents who participated in the EA. In this report, when we write blood levels of PFAS, we
are referring to the measurement of PFAS in the serum fraction of the blood. This report also
summarizes urine sample results from a subset of participants and presents results from the dust and
tap water samples. Finally, the relationships between blood results and the environmental sampling
data are explored. The Security-Widefield blood and urine results are compared to a nationally
representative sample of the US population. Specifically, ATSDR compared Security-Widefield data to
those collected by CDC as part of its National Health and Nutrition Examination Survey (NHANES). The
NHANES survey collects blood and urine samples from a representative sample of the civilian non-
institutionalized U.S. population and tests them for chemicals, including PFAS. PFAS levels are also
shown by age, race/ethnicity, sex, number of years living in the community, drinking water consumption
patterns, and other exposure parameters.
1
The laboratory reports branched and linear isomers of PFOA and PFOS in blood and urine. ATSDR reports on the
sum of the individual isomer concentrations of PFOA and PFOS.

ES-3
The samples were collected and analyzed in accordance with ATSDR’s Exposure Assessment Protocol:
Biological and Environmental Sampling of PFAS (EA protocol) to ensure their quality. This EA was
designed to estimate geometric mean concentrations of PFOS in blood for the sampling frame (i.e., the
Security-Widefield area served by the drinking water systems of the Security WD, Security MHP, and the
western portion of the Widefield WSD) population, with a precision goal of 15% or less. The precision is
a measure of how wide the confidence interval is around the estimated geometric mean. ATSDR met
this goal for PFOS, and precision for all PFAS measured in this EA ranged from approximately 3.9% to
16%. ATSDR also calculated geometric means that were adjusted to the age distribution of the sampling
frame population to correct for participation bias and to provide an estimate that is more generalizable
to the sampling frame community. ATSDR also calculated geometric means that were adjusted to the
national age distribution for comparison with the 2015–2016 NHANES survey. To assess possible
relationships between blood levels and various demographic and exposure variables, ATSDR used
statistical models. Univariate statistics, which evaluate one variable at a time, were used as a tool to
examine the data broadly and find patterns within the data. Multivariate statistics and regression
modeling were used to simultaneously account for multiple variables and to control for potential
confounding factors.
2
In this report we use the term ‘average’ to refer to the national age-adjusted
geometric mean.
Security-Widefield Community-Wide Findings
Finding 1. Average blood levels of PFHxS and PFOA in the Security-Widefield EA site
participants are higher than national levels. Averages of other PFAS were not higher than the
national levels or were detected too infrequently to compare to national levels.
Geometric means (i.e., averages) for PFHxS and PFOA blood levels were statistically higher (p<0.05) in
Security-Widefield EA participants when compared to CDC’s NHANES (2015–2016) testing, which was
limited to people over 12 years old. The statistically higher blood PFAS levels were observed for both
unadjusted geometric means for all EA participants and geometric means adjusted to the age
distribution of the U.S. population from NHANES 2015–2016.
Of the PFAS analyzed in blood, PFHxS had the largest elevations when compared to national levels. The
age-adjusted geometric mean blood PFHxS level among EA participants was 6.8 times the national level.
Blood PFHxS levels were above the national geometric mean for 96% of the Security-Widefield EA
participants and above the NHANES 95
th
percentile for 75% of the participants. The age-adjusted
geometric mean blood PFOA level was 1.2 times the national level.
Other PFAS measured in this EA (PFOS, PFNA, PFDA) were not higher than national levels. ATSDR was
unable to compare the geometric mean MeFOSAA levels because MeFOSAA was detected in less than
60% of NHANES samples. PFUnA was detected in less than 60% of the EA participant samples; due to the
large percentage of samples below the limit of detection, geometric means were not calculated.
Finding 2. Elevated blood levels of PFHxS and PFOA may be associated with past drinking
water contamination.
PFHxS, PFOS, and PFOA were detected in Security-Widefield water systems as early as 2013, though
contamination likely began earlier. Two of these PFAS (PFHxS and PFOA) had statistically elevated blood
2
A confounding variable is a factor that may distort or mask the relationship between a potential predictor and
measure of exposure.
ES-4
levels compared to national geometric means. The maximum concentrations observed in drinking water
in Security-Widefield water systems were 590 ppt for PFHxS, 210 ppt for PFOS, and 90 ppt for PFOA.
By November 2016, actions taken by the three affected water systems reduced PFAS levels in drinking
water below EPA’s HA for PFOS and PFOA. Before 2016, PFAS-containing AFFF were primarily
formulated with PFOS, but also contained various PFAS precursors that could break down in the
environment into other PFAS, such as PFHxS, which could explain the elevated blood PFHxS levels.
PFHxS and PFOA have very long biological half-lives (on the order of years). There were 3 years and 10
months between when the water systems took action to reduce exposure to contaminated drinking
water and collection of biological samples during the EA. Because of the long half-lives of PFHxS and
PFOA, past drinking water exposures may have contributed to the EA participants’ blood levels. PFHxS
has the longest estimated half-life of the three compounds (up to 35 years), which may contribute to
why it exceeded the NHANES 2015-2016 geometric mean by the largest margin.
PFHxS and PFOA were highly correlated in Security-Widefield EA participants’ blood (Pearson correlation
coefficient, r = 0.73). This means that, typically, residents who had elevated blood PFHxS levels also had
elevated blood PFOA levels. This correlation suggests a common exposure source, such as the pre-2017
Security-Widefield public drinking water supplies, though other sources of exposure may also have
contributed to the observed blood levels.
Additional observations from the multivariate analyses support the finding that past exposure to
contaminated drinking water may have contributed to the elevated blood levels.
• First, a consistent and statistically significant predictor of participant blood levels for PFHxS and
PFOA was how long the resident had lived in Security-Widefield during the past 20 years. Each
year of residence in the sampling frame over the past 20 years was associated with a 7.1%
increase in PFHxS levels and a 2.0% increase in PFOA levels.
• Second, adults who reported not drinking tap water at all at home on average had statistically
lower PFHxS (36%) and PFOA (24%) blood levels when compared to those who reported drinking
tap water at home with no filter or treatment device.
Multivariate models conducted separately for males and females suggest differences in the associations
(between blood levels and residency duration/tap water consumption) between males and female
participants.
Taken together, the data suggest that past drinking water exposure contributed to the elevated blood
levels of PFHxS and PFOA observed in the Security-Widefield EA participants.
Finding 3. Age, sex, occupational exposure, kidney disease history, local fruit and vegetable
consumption, and home cleaning frequency were associated with some PFAS blood levels.
PFAS blood levels varied with different demographic and exposure characteristics of the participant
population. The following relationships were statistically significant in multivariate analyses in the
Security-Widefield EA dataset in adult participants:
• Blood levels of PFHxS, PFOS, and PFOA were higher in older participants, and the size of the
effect varied by sex for PFHxS. In males, blood levels for these compounds increased by 1.0% to
1.7% for every year of participant age. In females, blood levels for these compounds increased
by 1.0% to 2.5% for every year of participant age.
ES-5
• Males had statistically higher blood levels of PFHxS and PFOS than females. PFOS blood levels in
males were 42% higher than in females. For PFHxS, the difference between males and females
was larger in younger people. For example, 30-year-old males had higher blood PFHxS levels
than 30-year-old females by 70%. For 50-year-old males, this difference was reduced to 35%.
• Adult participants who reported at least one occupational exposure in the past 20 years on
average had lower PFHxS (28%) than adult participants who reported no occupational exposures
in the past 20 years. Although this result was the opposite of expected, it is based on a relatively
small sample of participants with occupational exposure and should be interpreted with caution.
• Adult participants who reported a history of kidney disease had PFHxS blood levels that were
39% lower than those who did not. This result is based on a relatively small sample of
participants self-reporting a history of kidney disease and should be interpreted with caution.
• Adult EA participants who reported any consumption of locally grown fruits or vegetables had
blood PFOS levels that were 52% higher compared to participants who reported no such
consumption. While PFOS levels were higher in participants who reported consuming local
produce compared to those who did not, PFOS blood levels were not elevated in the
community.
• Adult participants who reported cleaning their homes three times per week or more on average
had 24% higher PFOS blood levels than adult participants who reported cleaning their homes a
few times per month or less; however, PFOS blood levels were not elevated in the community.
A few associations were observed in children (<18 years) in univariate analyses, though many variables
could not be examined because of the small number of child participants (n=28). Because of the small
sample size, results should be interpreted with caution. Specifically, the longer a child was breastfed, the
higher blood levels of PFOS and PFOA compared to non-breastfed children, and children that reported
ever drinking formula reconstituted with tap water on average had blood PFHxS, PFOS, and PFOA levels
that were lower than children that reported never drinking formula reconstituted with tap water.
Infants born to mothers exposed to PFAS can be exposed in utero and while breastfeeding. However,
based on current science, the benefits of breastfeeding outweigh the risks for infants exposed to PFAS in
breast milk. The final report on all EA sites will include a more robust analysis of children.
Finding 4. Only one PFAS was detected in urine and at relatively low concentrations.
ATSDR analyzed 36 (10%) of the urine samples collected. Only perfluorobutanoic acid
(PFBA) was detected; it was detected in 2.8% of the 36 samples that were analyzed. ATSDR did not
analyze all participants’ urine samples because none of the species were detected in more than 60% of
the samples analyzed.
Finding 5. All Security-Widefield drinking water samples collected during the EA in 2020 met
the EPA’s HA for specific PFAS in drinking water.
This is based on 17 filtered and 17 unfiltered water samples collected in 18 households during the EA.
These results are consistent with recent data collected from the Widefield WSD, Security WD, and
Security MHP water systems.
Finding 6. Patterns and levels of dust contamination measured in participating EA households
are comparable to those reported in selected U.S. studies.
Among the PFAS detected most frequently in household dust samples, N-MeFOSE and PFOS were
measured at the highest average concentrations. No nationally representative comparison values are
available, but geometric mean and median concentrations for PFAS measured in dust collected in the
ES-6
small subset of participating households (n=18) were within the range of levels reported in a few
published studies of other U.S. communities (with or without known PFAS contamination). Of the PFAS
measured in this EA’s household dust samples, PFOA (r=0.46) and MeFOSAA (r=0.57) were statistically
correlated with the same PFAS measured in participants’ blood. The final report on all EA sites will
include a more robust comparison of PFAS measured in dust and blood.
Limitations
There are several limitations associated with this assessment.
• The random sampling recruitment method used for this EA was designed to measure blood PFAS
concentrations that were generalizable to all Security-Widefield residents who were customers
of the Security WD, Widefield WSD, or Security MHP. However, the EA participant sample may
not be fully representative of the community. Only 6.3% of the households from the random
sample participated in the EA. Participant characteristics were different than those of the area’s
overall population. Participants were older, more likely to identify as White, and less likely to
identify as more than one race. ATSDR addressed some of these differences by calculating
geometric mean estimates that were adjusted to the age distribution of the community.
• Measurement of blood, urine, and environmental PFAS concentrations in EA participants may
improve the understanding of exposure in this community but will not provide information
about all sources of exposure. Additionally, identifying every potential confounding exposure is
not possible.
• There are challenges in measurement of trace levels of PFBA in urine, including selectivity of the
analytical instrumentation and potential for external contamination. Therefore, we advise
caution when interpreting the PFBA results in urine.
• Multivariate regression models explained a small to moderate portion of the variability in
participants’ blood PFAS levels (R-squared or R
2
, a measure of model goodness-of-fit, ranged
between 0.13 and 0.30 in all-adult models). This means that other factors not identified could
influence the relationships reported in this assessment (see “Statistical Analysis” section for
details).
• This EA did not directly assess participants’ tap water consumption prior to the reduction of
PFAS in the municipal water systems.
• This EA was not designed to investigate health problems associated with exposure to PFAS.
Without additional information about exposure-response relationships, the results of this EA
cannot be used to assess current or past health problems or predict the future occurrence of
disease. PFAS found in a person’s blood or urine means that exposure has occurred. The
presence of PFAS in blood or urine does not tell us how, where, when, or for how long a person
was exposed to PFAS. Exposure to PFAS does not mean adverse health effects will result, either
now or in the future.
• The dust results are exploratory and should be interpreted with caution. They are based on a
limited set of samples, and in some cases those samples are based on a small sample mass.
Recommendations
This PFAS EA provides evidence that past exposures to PFAS in drinking water have impacted the levels
of PFAS in people’s bodies. These PFAS are eliminated from the body over a long period of time. This
allowed ATSDR to measure PFAS even though exposures through drinking water were mitigated, or
lowered, years ago.

ES-7
Although the exposure contribution from PFAS in drinking water in Security-Widefield has been
mitigated, there are actions community members and county officials can take to further reduce
exposures to PFAS and protect public health.
Based on the PFAS drinking water test results from drinking water wells in Security-Widefield, ATSDR
does not recommend an alternate source of drinking water at this time.
1. What the Security WD, Widefield WSD, and Security MHP can/should do:
a. Operators of these three public water systems should continue to monitor concentrations of
PFAS in drinking water delivered to the Security-Widefield community to ensure that
concentrations of PFAS remain below the EPA’s HA or other applicable guidelines for specific
PFAS in drinking water. Results of PFAS monitoring should be shared with community
members through appropriate communication channels (Consumer Confidence Reports for
Security WD: http://securitywsd.com/water-quality/; Consumer Confidence Reports for the
Widefield WSD, https://www.wwsdonline.com/consumer-confidence-report).
b. All treatment systems to remove PFAS from the municipal drinking water in Security-
Widefield should be maintained appropriately to ensure that PFAS concentrations remain
below the EPA’s HA or other applicable guidelines for specific PFAS in drinking water.
2. What community members can/should do:
a. Become familiar with Consumer Confidence Reports for information on water quality in
Security-Widefield (Consumer Confidence Reports for Security WD:
http://securitywsd.com/water-quality/; Consumer Confidence Reports for the Widefield
WSD, https://www.wwsdonline.com/consumer-confidence-report).
b. Private well owners living in the area affected by PFAS should consider having their wells
tested for PFAS if testing has not been conducted before. To learn more about testing wells
for PFAS visit:
https://www.elpasocountyhealth.org/news/news-release/2019/resources-
for-pfc-water-contamination-and-testing. Global public health organization NSF
International has developed a test method to verify a water filter’s ability to reduce PFOA
and PFOS to below the health advisory levels set by the EPA. NSF International-approved
devices can be found at: https://info.nsf.org/Certified/DWTU/ Click on “reduction devices”
at the bottom of the page for PFOA and PFOS.
c. Nursing mothers should continue breastfeeding. Based on current science, the known
benefits of breastfeeding outweigh the risks for infants exposed to PFAS in breast milk.
d. When possible, eliminate or decrease potential exposure to PFAS in consumer products,
such as stain-resistant products and food packaging materials. To learn more visit:
https://www.fda.gov/food/chemical-contaminants-food/questions-and-answers-pfas-food
e. Pay attention to advisories about food consumption, such as local fish advisories.
f. Discuss any health concerns or symptoms with your health care provider. Share results of
PFAS blood testing with your health care provider and make them aware of ATSDR
resources for clinicians (https://www.atsdr.cdc.gov/pfas/resources/info-for-health-
professionals.html). Follow the advice of your health care provider and the
recommendations for checkups, vaccinations, prenatal care, and health screening tests.
g. At this time, ATSDR does not have plans to conduct additional blood testing for PFAS nor
recommend PFAS EA participants get individually retested for PFAS in blood. The biological
half-lives of many of the PFAS measured in people’s blood are long. PFHxS has one of the
longest half-lives. This means that PFAS blood levels are not expected to change significantly

ES-8
in the near-term, even if exposure stops. Additionally, it is unclear what an individual’s PFAS
test results mean in terms of possible health effects.
For the general population blood tests for PFAS are most useful when they are part of a
scientific investigation like this EA. Test results will tell you how much of each PFAS is in your
blood, but it is unclear what the results mean in terms of possible health effects. In addition,
blood testing for PFAS is not a routine test offered by most doctors or health departments. If
you are concerned about the effect of PFAS on your health, talk to your health care provider
and make them aware of ATSDR resources for clinicians
(https://www.atsdr.cdc.gov/pfas/resources/info-for-health-professionals.html
).
h. ATSDR is funding a multi-site health study, including one site in the El Paso County area
called the Colorado Study on Community Outcomes from PFAS Exposure (CO-SCOPE). The
CO-SCOPE is being conducted by the same investigative team that completed the PFAS
AWARE study. The study will evaluate PFAS levels in serum as well as health markers and
neurobehavioral outcomes in children. If you are interested in being included in the study or
want further information, please contact
Fountain Valley PFAS Study | PFAS Multi-Site Study
Colorado: CO SCOPE (co-scope.org)
i. Follow the advice of your child’s health care provider and the recommendations for well
child checkups, vaccinations, and recommended health screening tests. Consult
https://health.gov/myhealthfinder
to help identify those vaccinations and tests.
j. For additional information about environmental exposures and children’s health, contact
the Pediatric Environmental Health Specialty Units, a nationwide network of experts in
reproductive and children’s environmental health (https://www.pehsu.net/
).
For More Information
If you have questions or comments or want more information on the Security-Widefield EA site, call
800-CDC-INFO or email [email protected]v. For more information on the work CDC/ATSDR is doing to address
PFAS exposure, visit ATSDR’s PFAS website: https://www.atsdr.cdc.gov/pfas/. For other EA or PFAS-
related questions, email [email protected].

1
Background and Purpose
The Centers for Disease Control and Prevention (CDC)
and the Agency for Toxic Substances and Disease
Registry (ATSDR) are conducting exposure
assessments (EAs) in communities near current or
former military bases that are known to have had per-
and polyfluoroalkyl substances (PFAS) in their drinking
water. One of these communities is Security-Widefield
in El Paso County, Colorado. This report summarizes
the findings of the Security-Widefield EA. When all
EAs are complete, ATSDR will prepare a report
describing the results across all sites.
The EA involved collecting responses to exposure
history questionnaire responses, biological samples
(blood and urine), and environmental samples (tap
water and household dust). ATSDR collected biological samples at the Security Village Fire Station
between September 15 and September 28, 2020. During this same time frame, ATSDR administered
questionnaires over the phone and took water and dust samples in a subset of randomly chosen
participant homes.
The results of the EA:
The EA does not look at what types of health problems are associated with exposure and is not meant to
determine if PFAS levels in blood or urine are risk factors for illness now or later in life. Additionally, the
EA does not tell us exactly how or where people were exposed or when or how long PFAS exposure
lasted.
ATSDR’s Exposure Assessment Protocol: Biological and Environmental Sampling of PFAS, termed the
PFAS EA Protocol [ATSDR 2019a], provides additional background, describes the criteria for selecting
communities for the EAs, and highlights the procedures ATSDR used in conducting the EAs.
What Are PFAS?
Human exposure to PFAS is a growing environmental health concern. PFAS are synthetic chemicals used
in many industries and consumer products since the 1950s. They have been used in nonstick cookware;
water-repellent clothing; stain-resistant fabrics and carpets; cosmetics; firefighting foams; and products
• tell us the amount of PFAS in the blood of individual participants and the Security-Widefield
community and how these levels compare to the general U.S. population,
• tell us the amount of PFAS in the urine of individual participants and the EA community and how
these levels compare to the general U.S. population,
• provide a better understanding of environmental factors that affect PFAS exposure,
• provide information that may be used to stop or reduce PFAS exposure,
• produce information that public health professionals can use to help communities affected by
PFAS, and
• inform future studies looking at the effect of PFAS exposure on human health.
Exposure assessment (EA) participants were
recruited among El Paso County residents
living near the Peterson Air Force Base who
received drinking water from the Security
Water District, western portions of the
Widefield Water Sanitation District, or
Security Mobile Home Park that had PFAS
levels above state or federal guidelines. For
purposes of this report, we refer to the
“Security-Widefield EA” to describe the EA
conducted in this area. For more
information and a map of the area see the
“Methods” section of the report.
2
that resist grease, water, and oil [Buck et al. 2011; Gluge et al. 2020; Wang et al. 2017]. Exposure to
PFAS has been associated with increased cholesterol, decreased vaccine response in children, changes in
liver enzymes, small decreases in infant birth weights, increased risk of high blood pressure or pre-
eclampsia in pregnant women, and increased risk of kidney and testicular cancer [ATSDR 2021].
There are thousands of different PFAS. This assessment discusses some of the most commonly studied
PFAS, which include perfluorooctanoic acid (PFOA), perfluorooctane sulfonic acid (PFOS),
perfluorohexane sulfonic acid (PFHxS), perfluorononanoic acid (PFNA), perfluorodecanoic acid (PFDA),
and perfluoroundecanoic acid (PFUnA). The manufacture and import of PFOA, precursor chemicals that
can break down to PFOA, and related higher homologue chemicals, have been mostly phased out in the
United States. However, existing stocks of PFOA might still be used, and there might be PFOA in some
imported articles. PFOS manufacture in the United States has not been reported to the EPA since 2002,
however, there are some limited ongoing uses of PFOS. These PFAS with long perfluoroalkyl chains are
no longer produced in the United States because of concerns over their high persistence, tendency to
bioaccumulate, and potential risks to human health and the environment. Other countries may still
manufacture and use them, but U.S. manufacturers have replaced these compounds with shorter
chained PFAS, or chemicals with alternative chemistries, such as GenX (HFPO-DA), which typically have
shorter biological half-lives. Some of the PFAS discussed in this report, such as N-methyl
perfluorooctanesulfonamidoacetic acid (MeFOSAA), are considered precursors that can degrade in the
environment or in people to other PFAS [ATSDR 2021; Wang et al. 2017].
PFAS do not occur naturally but are widespread in the environment. PFAS can be released into the
environment during their production, use, or disposal. PFAS have been found in soil, sediment, water,
animal and plant life, and air. Most PFAS (including PFOA, PFOS, PFHxS, and PFNA) are either very
resistant to breaking down or degrade into other PFAS that do not degrade further. Certain PFAS will
therefore remain in the environment indefinitely. Most people in the United States have been exposed
to PFAS. At least one PFAS was detected in more than 99% of NHANES samples (1999-2000 survey cycle)
[Calafat et al. 2007a]. Exposure can occur via contaminated drinking water for which ingestion is
believed to be the primary exposure route. Studies have shown that showering, bathing, and swimming
in water containing PFAS at levels seen in Security-Widefield are not expected to be an important
contributor to PFAS exposure relative to the contribution from drinking water [Sunderland 2019].
ATSDR’s PFAS EAs focused on communities with known exposures via contaminated drinking water.
However, residents may have had additional exposures to PFAS, such as the following [Sunderland
2019]:
• eating food packaged in materials containing PFAS (e.g., popcorn bags, fast food containers,
pizza boxes)
• eating fish or shellfish caught in PFAS-contaminated waters
• using consumer products such as stain-resistant carpeting and water-repellent clothing
• eating garden vegetables grown with PFAS-contaminated water or soil
• accidentally swallowing PFAS-contaminated soil
• drinking infant formula mixed with PFAS-contaminated water
• consuming breastmilk from women exposed to PFAS
• gestational exposure to PFAS
• working in industries that manufacture, process, or use products containing PFAS
• background exposure to PFAS due to their ubiquitous nature.

3
ATSDR asked study participants about these types of potential exposures to evaluate whether these
exposures might influence PFAS levels in the EA communities.
After PFAS enter the human body, some PFAS can remain there for a long time. Most studies estimate a
half-life of PFHxS between 4.7 and 8.5 years, although some have estimated half-lives as long as 35 years
[ATSDR 2021]. Most half-life estimates for PFOS are between 3.3 and 7.4 years, with a maximum of 27
years [ATSDR 2021]. For PFOA, most studies estimate the half-life between 2.1 and 3.9 years with a
maximum of 10.1 years [ATSDR 2021].
The body of science about PFAS exposure and health effects is growing rapidly. Some, but not all,
scientific studies have shown that exposure to certain PFAS may be linked to harmful health effects.
While this EA does not examine specific health outcomes associated with PFAS exposure, EA findings
might help inform future studies on how PFAS exposure affects human health.
Why Security-Widefield?
Security-Widefield was one of several sites located near military installations with identified PFAS
drinking water contamination from use of products such as aqueous film forming foam (AFFF). When
selecting EA sites, ATSDR considered the extent of PFOA and PFOS contamination in drinking water
supplies, the duration over which exposure may have occurred, and the number of potentially affected
residents.
3
PFAS and precursors that degrade to other compounds measured in this EA were used in historical AFFF
formulations. Two types of PFAS containing AFFF were manufactured before 2016 [ITRC 2020]. Both
formulations contained PFAS or PFAS precursors, the use of which resulted in the release of PFOS,
PFHxS, PFOA, and PFHxA into the environment. Possibly as early as the 1970s, Peterson Air Force Base
(the Base) used AFFF containing PFAS for its firefighter training (AFCEC 2018). Over time, the PFAS from
the AFFF moved off site in groundwater and contaminated nearby public drinking water supply wells.
When PFAS first entered Security-Widefield’s public water systems is not known. These substances were
first detected in municipal wells near the Base in 2013 and 2014, through testing conducted for the U.S.
Environmental Protection Agency’s (EPA’s) Third Unregulated Contaminant Monitoring Rule (UCMR 3)
[EPA 2017]. The rule required testing for six PFAS. The levels measured in the Security Water District
(WD) and Widefield Water and Sanitation District (WSD) water systems during UCMR 3 were above
EPA’s provisional health advisory, which at the time was 400 parts per trillion (ppt) for PFOA and 200 ppt
for PFOS.
• In the Security WD system, PFHxS, PFOS, or PFOA were detected in 36 out of 38 samples taken
between January 14 and August 11 of 2014. Wells from both the eastern and western parts of
the system exceeded EPA’s provisional health advisory, and the highest PFOA+PFOS
concentration was 1,370 ppt in a well in the eastern part of the system. However, water from
this well fed into a tank and mixed with uncontaminated surface water prior to entering the
distribution system. According to Security WD engineers, on average, the groundwater would
have been diluted with uncontaminated surface water by approximately 90 percent. The highest
measurements of finished individual PFAS in finished water (water consumed by customers) in
the Security WD system were 590 ppt for PFHxS, 210 ppt for PFOS, and 90 ppt for PFOA.
3
PFHxS data were not available for all sites evaluated so were not considered in the site selection process even
though water contaminated by AFFF often has higher concentrations of PFHxS than PFOA or PFOS.

4
• In the Widefield WSD system, PFHxS, PFOS, or PFOA were detected in 11 out of 17 samples
taken between November 12, 2013, and August 11, 2014. PFOA+PFOS exceeded EPA’s health
advisory in five samples with a maximum concentration of 246 ppt at a well in the western part
of the system. Water that entered the eastern part of the Widefield WSD distribution system
was less contaminated. The highest measurements of individual PFAS in the Widefield WSD
system, detected in western portions of the system, were 330 ppt for PFHxS, 210 ppt for PFOS,
and 48 ppt for PFOA.
In 2016, EPA issued a lifetime health advisory (HA) for the sum of PFOA and PFOS levels in drinking
water (70 ppt). In 2016 and 2017 (CDPHE, 2019) the Colorado Department of Public Health and
Environment (CDPHE) reported the results of PFAS testing in water supplies across El Paso County. The
CDPHE data confirmed PFAS contamination throughout the Security WD distribution system and in the
western parts of the Widefield WSD system. The CDPHE data showed exceedances of the EPA’s HA in a
third system, the Security Mobile Home Park (MHP).
• In February 2016, PFAS was detected in an active groundwater well within the Security MHP
system at levels of 70 ppt for PFOS and 33 ppt for PFOA.
Between January and November of 2016, Security WD and Widefield WSD inactivated their
contaminated groundwater wells and shifted to uncontaminated surface water sources. In 2017,
Widefield WSD installed an ion exchange system to treat PFAS in water from its contaminated wells.
Security WD currently uses uncontaminated surface water sources. Residents of Security MHP were
provided bottled water beginning in the summer of 2016 until a treatment system was installed in
November of 2017. By 2016, all three systems had taken active measures to reduce PFAS exposure to
customers.
The information available to ATSDR indicates that, when the EA was conducted in 2020, drinking water
supplies in Security-Widefield met or were below the EPA’s HA for PFAS in drinking water.
Methods
ATSDR’s PFAS EA protocol [ATSDR 2019a] details the approaches used to recruit participants, collect
samples, administer exposure history questionnaires, and evaluate data. This section briefly describes
how those methods were applied to the Security-Widefield EA.
Sampling Frame
This EA targeted a specific geographic area, called the sampling frame or sampling area. The sampling
frame for this EA was the area served by the drinking water systems of Security WD, Security MHP, and
the western portion of the Widefield WSD (see Figure 1
). Based on a review of El Paso County land
parcel data, ATSDR determined that 10,783 households in the sampling frame were connected to the
Security-Widefield water supplies. These households formed the sampling frame from which households
were randomly selected for recruitment. Households with private wells were not eligible for
participation. Private well owners living in the area affected by PFAS should consider having their wells
tested for PFAS if testing has not been conducted before. To learn more about testing wells for PFAS
visit:
https://www.elpasocountyhealth.org/news/news-release/2019/resources-for-pfc-water-
contamination-and-testing.

5
Figure 1. Sampling frame for the Security-Widefield Exposure Assessment

6
Participant Eligibility
Security-Widefield residents who were randomly selected to participate and met the following criteria
were eligible to participate in the EA:
• Lived within the sampling frame (i.e., Security-Widefield households in the affected area shown
in Figure 1
) for at least one year before November 10, 2016, which is when Security-Widefield
reduced PFAS drinking water concentrations below EPA’s HA in all three water systems.
• Were at least 3 years old at the time of recruitment. This age criterion was used because
national reference values are not available children under the age of three.
• Did not have bleeding disorders and were not anemic, unless they confirmed with their doctor
the ability to safely provide a blood sample.
People potentially exposed to PFAS occupationally, such as firefighters, active-duty military, and
veterans were able to participate if they met the three eligibility criteria. Participants did not receive
incentives and paid no costs to participate.
Participant Recruitment
ATSDR randomly selected 3,000 households in the
sampling frame for recruitment. This number was chosen
to attempt to achieve the protocol recruitment target of
395 participants. Every household had an equal chance of
being selected, and all members of randomly selected
households who met eligibility criteria were invited to
participate. This type of recruitment, called a one-stage
cluster sampling design, means that a single household
may have multiple participants.
Recruitment was done through mailings, phone calls, and in-person visits to households that could not
be reached by phone. Each household for which ATSDR had a phone number received a minimum of
three recruitment call attempts. In each attempt, ATSDR called all working phone numbers (cell phone
and landline) associated with a household. For calls that went to voicemail, ATSDR staff left messages
encouraging residents to call back to schedule appointments. Door-to-door recruitment occurred after
each household had received an initial outreach letter and at least one recruitment call attempt.
Results from the randomly selected participants can provide information about community-level
exposure. Had ATSDR accepted volunteers, results could not be used to estimate exposure across the
Security-Widefield sampling frame. After two waves of recruitment (initially reaching out to 1,162
households and later reaching out to an additional 1,838 households), 384 residents from 200
households scheduled appointments for biological sampling and questionnaire completion.
ATSDR attempted to recruit 10% of the participating households for environmental sampling. ATSDR
invited 30 households, and 20 households scheduled environmental sampling appointments.
Data Collection and Analysis
The Security-Widefield EA involved collection of three types of data: questionnaires, biological samples
(blood and urine), and environmental samples (tap water and household dust). The ATSDR project team
collected biological samples at the Security Village Fire Station between September 15 and September
Measuring PFAS in the blood of people
from randomly selected households
allowed ATSDR to estimate exposure
to PFAS from public drinking water for
the entire community (the sampling
frame) in the affected area, even those
who were not tested.

7
28, 2020. During this same time frame, ATSDR administered questionnaires over the phone and
collected environmental samples in a subset of randomly chosen participant homes. All data met the
stringent quality control requirements for sample collection and analysis.
Before any data collection, ATSDR obtained written consent from the participants. The purpose of the
consent process was to ensure participants were fully aware of the purpose of the EA, sample collection
procedures, benefits and risks of participating, and privacy protections. Copies of consent forms are
included in the PFAS EA Protocol.
ATSDR project staff handled all data collected in accordance with the Standard Operating Procedures of
PFAS Exposure Assessment Data Management [ATSDR 2019b]. These procedures have very strict
requirements for handling any personally identifiable information. ATSDR project staff protected this
information to the extent required by federal and Colorado law. All signed consent forms were mailed to
and are securely archived at ATSDR headquarters. Participant responses to phone questionnaires were
logged directly into ATSDR’s secure data network. All information provided by participants was kept
confidential, and no personally identifiable information appears in any of ATSDR’s public reports for this
site.
Table 1
, at the end of this section, provides more details on the number of participants enrolled and the
final number of samples collected during this EA. Table 2 lists the PFAS measured in the EA’s biological
and environmental samples.
Biological Sampling and Questionnaire Administration
Of the 384 residents who scheduled data collection appointments, 359 (93%) participated in the EA.
ATSDR administered exposure history questionnaires to 355 EA participants: 321 for adults 18 and older,
and 34 for children between the ages of 3 and 17. Four participants that provided blood samples did not
complete a questionnaire. ATSDR used one questionnaire for adults and another for children. Both
addressed topics relevant to PFAS exposure, such as residential and work histories, drinking water
habits, and use of PFAS-containing consumer products.
A phlebotomist collected blood samples from all 359 participants. ATSDR processed the blood samples
in the field, aliquoting the serum portion of the blood.
After the sampling was complete and upon further review of each participant’s residential history,
ATSDR determined that 13 participants had not lived in the sampling frame for at least one full year
before November 10, 2016, and therefore were not eligible for the study. Questionnaire and biological
data for these participants were excluded from the data evaluation, but ATSDR sent them their
individual results. This means that a total of 346 blood samples (318 adults and 28 children) were
considered in the community exposure summary. These samples were collected from participants
residing in 188 unique households. This represents a household participation rate of 6.3% (i.e., 6.3% of
the 3,000 recruited households had at least one person participate in the EA).
Urine samples were collected from 354 participants (324 adults and 30 children). Per the EA protocol,
10% of the urine samples were randomly selected for initial analysis. ATSDR randomly selected 36
samples for analysis. These samples were collected from participants (34 adults and 2 child) who resided
in 36 unique households.
CDC’s National Center for Environmental Health laboratory analyzed the serum portion of blood and
urine samples for the suite of PFAS measured in the 2015–2016 National Health and Nutrition
8
Examination Survey (NHANES) [CDC 2019]. As part of NHANES, CDC takes biological samples and tests
them for chemicals, including PFAS, from a representative sample of 5,000 people across the country
during each two-year cycle. All laboratory analyses followed established procedures for quality
assurance and control according to the Center’s methodology.
During the consent process, participants were given the option to allow ATSDR to store biological
samples for potential future PFAS analysis. Blood and urine samples from participants who provided this
consent are being stored frozen at CDC for potential future analysis.
Environmental Sampling
ATSDR collected tap water and dust samples from 18 of the 20 households that had initially scheduled
appointments. Two households were unavailable to complete their environmental sampling
appointment. At each participating household, ATSDR collected a drinking water sample from the
kitchen tap. If point-of-use filtration was in place, ATSDR project staff attempted to collect a sample
before and after filtration. Tap water samples were collected and analyzed in accordance with EPA’s
Method 537.1: Determination of Selected Per- and Polyfluorinated Alkyl Substances in Drinking Water by
Solid Phase Extraction and Liquid Chromatography/Tandem Mass Spectrometry [Shoemaker and
Tettenhorst 2018].
Project staff also collected a composite dust sample from the floor at a minimum of three locations
inside each selected home: the primary living space as identified by the homeowner (e.g., living room,
family room, television room), the kitchen, and the bedroom in which participants reported spending
the most time. Dust collection was intended to generate more information about the contribution of
non-drinking-water exposures to overall PFAS exposure. Participants were instructed not to vacuum
carpeting or sweep floors for five days prior to the scheduled visit. Adapting methods described in Scher
et al. [2018], ATSDR collected dust samples using a high-volume air sampler connected to an open-faced
37 millimeter filter cassette with an 0.8 micron filter. A wooden 2 square foot (ft
2
) sampling template
was used to mark off each sampling area. ATSDR project staff attempted to collect at least 1 gram of
dust in the open-faced cassettes from each home by vacuuming the same 2 ft
2
surface at least four
times with the cassette (vertically, horizontally, and in circles). Samples were taken preferentially from
mats, carpets, and area rugs. Household dust samples were analyzed in accordance with SGS AXYS
Method MLA-110 (revision 01, version 06), Analytical Procedure for the Analysis of Per- and
Polyfluoroalkyl Substances (PFAS) in Aqueous Samples, Solids and Solvent Extracts by LC-MS/MS [SGS
AXYS 2019].
The environmental samples collected during the EA were consumed in the analytical process and are not
available for potential future analysis.

9
Table 1. Summary of recruitment and data collection efforts
Recruitment
Households invited to participate by mail 3,000
Wave 1 of recruitment 1,162
Wave 2 of recruitment 1,838
Households reached by mail 2,567
Households reached by phone 1,147
Household door-to-door visits 2,640
Biological sampling:
Individuals enrolled 384
Households enrolled 200
Environmental sampling:
Households invited 30
Households enrolled 20
Data Collection
Completed questionnaires 355
Adults 321
Children 34
Blood samples
Included in community statistics (188 households) 346
Adults 318
Children 28
Urine samples
Collected 354
Adults
324
Children 30
Included in community statistics (36 households) 36
Adults 34
Children 2
Dust samples collected and analyzed (one composite
sample per household)
18
Tap water samples collected and analyzed (18 households) 34
Filtered 17
Unfiltered 17

10
Table 2. List of PFAS measured for in blood, urine, tap water, and dust
PFAS
Abbreviation
PFAS Chemical Name
Measured
in Blood?
Measured
in Urine?
Measured
in Water?
Measured
in Dust?
PFBS perfluorobutane sulfonic acid
PFPeS perfluoropentane sulfonic acid
PFHxS perfluorohexane sulfonic acid
PFHpS perfluoroheptane sulfonic acid
PFOS perfluorooctane sulfonic acid
n-PFOS sodium perfluoro-1-octanesulfonate
Sm-PFOS
mixture of sodium perfluoro-5-methylheptane
sulfonate isomers
PFNS perfluorononane sulfonic acid
PFDS perfluorodecane sulfonic acid
PFDoS perfluorododecanesulfonate
PFBA perfluorobutanoic acid
PFPeA perfluoropentanoic acid
PFHxA perfluorohexanoic acid
PFHpA perfluoroheptanoic acid
PFOA perfluorooctanoic acid
n-PFOA ammonium perfluorooctanoate
Sb-PFOA
mixture of perfluoro-5-methylheptanoic acid
isomers
PFNA perfluorononanoic acid
PFDA perfluorodecanoic acid
PFUnA perfluoroundecanoic acid
PFDoA perfluorododecanoic acid
PFTrA perfluorotridecanoic acid
PFTA perfluorotetradecanoic acid
PFOSA perfluorooctanesulfonamide
N-MeFOSA N-methylperfluorooctanesulfonamide
MeFOSAA
N-methyl perfluorooctanesulfonamidoacetic
acid
N-MeFOSE N-methylperfluorooctanesulfonamidoethanol
N-EtFOSA N-ethylperfluorooctanesulfonamide
N-EtFOSAA N-ethyl perfluorooctanesulfonamidoacetic acid
N-EtFOSE N-ethylperfluorooctanesulfonamidoethanol
FtS 4:2 fluorotelomer sulfonic acid 4:2
FtS 6:2 fluorotelomer sulfonic acid 6:2
FtS 8:2 fluorotelomer sulfonic acid 8:2
HFPO-DA
(GenX)
hexafluoropropylene oxide dimer acid
DONA 4,8-dioxa-3H-perfluorononanoic acid
9Cl-PF3ONS
9-chlorohexadecafluoro-3-oxanone-1-sulfonic
acid
11Cl-PF3OUdS
11-chloroeicosafluoro-3-oxaundecane-1-
sulfonic acid

11
Statistical Analysis
The EA Protocol describes the statistical methods
used. Briefly, the data objectives of this EA were to
(1) estimate geometric mean concentrations of PFAS
in the sampling frame population (with a precision
target of at least 15% and a 5% level of significance
for PFOS), (2) compare community level data to
national levels, and (3) explore relationships
between questionnaire data and measured biological
and environmental data.
ATSDR processed the PFAS sampling results in two
ways before performing statistical analyses:
• First, ATSDR substituted all non-detect
observations with a value equal to the limit
of detection (LOD) divided by the square root
of 2. (A non-detect result means the sample
did not contain enough PFAS to be reliably
measured by this project’s highly sensitive
laboratory methods.) This substitution
method is consistent with that applied in
CDC’s NHANES. Note that Appendix B
provides the results of a sensitivity analysis
exploring alternate substitution approaches.
• Second, ATSDR calculated the total PFOA and
total PFOS concentrations measured in each
blood and urine sample. The laboratory
reports two different measurements for
PFOA and PFOS. For PFOA, the laboratory
reports the amount of branched PFOA (Sb-
PFOA) measured in the sample separate
from the amount of linear PFOA (n-PFOA) in
the same sample. ATSDR summed these
values and performed statistical analyses
using total PFOA results. Similarly, ATSDR
calculated total PFOS by summing the linear
PFOS (n-PFOS) and branched PFOS (Sm-
PFOS) concentrations. These same
summation methods are applied to NHANES
data.
For blood and urine, ATSDR first calculated summary
statistics for each PFAS (i.e., frequency of detection,
maximum detected concentration, geometric mean,
95% confidence intervals around the geometric
mean, and 25
th
, 50
th
[median], 75
th
, 90
th
, and 95
th
percentiles). The protocol specified that geometric
Statistical Terms
Geometric mean: The geometric mean is a
type of average and provides an estimate of
the central point of a set of numbers. It is
often used for environmental data that
exhibit a skewed distribution (e.g., a dataset
with several values that are much higher
than the rest of the results). The geometric
mean is less influenced by high values than
an arithmetic mean.
Percentiles (25th, 50th, 75th, 90th, 95th): A
percentile provides additional information
about the distribution of a dataset and
represents the value below which a certain
percentage of the data fall. For example, a
95th percentile of 25 micrograms per liter
(µg/L) indicates that 95% of results fall below
this concentration.
Confidence intervals: A confidence interval
defines a range of values that's likely to
include a specific value with a certain degree
of confidence (probability). It provides a
measure of how much uncertainty there is
with any particular statistic In this EA, ATSDR
estimated geometric means for the PFAS
blood levels measured among study
participants. The 95% confidence interval
around the geometric mean represents the
range within which the true population
mean is expected to lie. More specifically, if
we hypothetically repeated the study 100
times, 95 times out of 100 the mean of the
sampling frame population would fall within
this range.
Precision: Precision provides information on
the reproducibility of a study and is
associated with sample size. The larger the
sample size the higher the precision. In the
context of this EA, precision was estimated
based on the width of confidence intervals
around the geometric mean. A wide
confidence interval indicates low precision
while a narrow confidence interval suggests
high precision.

12
means would be calculated if >=60% of samples had detections. Geometric means were calculated as
the measures of central tendency because of the lognormal distribution of blood and urine
measurements. Note that many of the statistics could not be calculated for urine due to the low
detection frequency.
One of the objectives of this EA was to estimate community-level exposures. While random recruitment
at the household level helps allow for such an estimation, ATSDR evaluated demographic differences
between the Security-Widefield EA participants and all residents in the sampling frame. This was done
for age, race, and ethnicity using a two-sample test for equality of proportions. To correct for
participation bias, ATSDR also calculated geometric means adjusted to the age distribution of the
sampling frame population using 2010 Census block data.
ATSDR compared community-level statistics for PFAS in blood to national PFAS data reported by CDC in
the 2015–2016 NHANES (i.e., for the EA sample population 12 years of age and older). To control for
differences in the age distribution, the EA geometric
means were adjusted to the age distribution of the U.S.
population during NHANES 2015–2016. Note that
NHANES 2017-2018 data were not available at the time
this report was originally drafted. For urine, ATSDR
compared community-level data to national-level data
from the 2013–2014 NHANES compiled by Calafat et al.
[2019], the only nationally representative data available
for PFAS in urine. ATSDR relied on two sample t-tests (on
log-transformed data) for these comparisons, using a p-
value of less than 0.05 to identify statistically significant
differences.
ATSDR then used information gathered in the exposure questionnaire to understand and quantify how
demographic data and other exposure characteristics relate to PFAS measurements in blood. For this,
ATSDR relied on self-reported information, such as age, race/ethnicity, sex, length of residency in the
sampling frame, tap water and food consumption patterns, and work/school history. All numerical
responses were treated as continuous variables. In some cases, categorical variables were collapsed
when there were too few responses (<10) in a given category. In order to explore sex-specific
associations (e.g., women having biological children [yes/no], having breastfed children [yes/no],
duration of breastfeeding), ATSDR also evaluated multivariate models for males and females only. For all
univariate and multivariate analyses, ATSDR modeled log transformed (logarithm base 10 or log
10
) blood
PFAS concentrations.
ATSDR did not conduct detailed statistical analyses for urine data because of low frequencies of
detection. ATSDR analyzed a subset of urine samples and found that, for all PFAS, the frequency of
detection was < 60%. The protocol specified that all urine samples would be analyzed if the geometric
mean calculated for any site exceeded the 95
th
percentile from NHANES. The protocol specified that
geometric means would be calculated if ≥60% of samples had detections, and the rest of the samples
would be analyzed if the calculated geometric mean exceeded the NHANES 95
th
percentile. Since no
PFAS were detected in 60% or more of the analyzed samples, no geometric means were calculated for
any PFAS in urine and ATSDR did not analyze the remainder of the urine samples. The 95
th
percentile
concentration for PFBA, was below the detection limit.
A p-value helps determine the
significance of the results of a statistical
test, such as the difference between
two means. The lower the p-value the
more likely the observed difference is
not due chance alone. In this report, a p-
value of less than 0.05 (p<0.05) is
described as statistically significant. This
level specifies less than a 5% probability
of being due to chance alone.

13
For tap water data, ATSDR compared PFAS levels measured with and without filtration to EPA’s HA value
(70 ppt for the sum of PFOA and PFOS). For dust, ATSDR calculated summary statistics and compared
results to those in selected peer-reviewed literature. ATSDR also evaluated correlations between PFAS
levels measured in household dust and blood collected from participants residing in homes where dust
samples were collected.
To account for the one-stage cluster design, ATSDR conducted all statistical analyses in SAS (release 9.4,
SAS Institute, Cary, NC) using complex survey procedures (e.g., SURVEYMEANS, SURVEYREG). To do this,
ATSDR assigned household IDs to all participants and calculated summary statistics while accounting for
clustering at the household level. For blood results across all EA participants, intra-cluster correlation
coefficients ranged from 0.26 to 0.81, suggesting weak to strong correlation of PFAS blood levels within
a household. Appendix B provides more information on clustering, as well as further details on the
statistical methods used for this EA and how results from this EA compared to the assumptions used to
estimate the target sample size of 395 participants.
Results
This section summarizes EA findings. It first profiles the Security-Widefield EA participants and compares
their demographics to the entire sampling frame, then reviews the blood, urine, tap water, and
household dust measurements that ATSDR collected. Those reviews use exposure history questionnaire
data to provide further context on the measurements. (The next section, “Discussion,” further evaluates
the observed trends using insights from the broader scientific literature on PFAS drinking water
exposures.)
Most analyses in this section reflect the entire Security-Widefield EA participant population, but some
pertain to subsets of that population. This is because separate exposure history questionnaires were
administered to adults and children and because some questions on the adult questionnaire only
applied to females.
Profile of Security-Widefield (El Paso County) EA Participants
EA participants responded to exposure history questions and reported information on many
characteristics, such as their age, sex, race/ethnicity, residential and occupational history, and drinking
water consumption. Table 3
summarizes this information.

14
Table 3. Characteristics of Security-Widefield EA participants
Characteristics
Count of EA
Participants (n)*
Percent of EA
Participants (%)
‡
Adults and children combined
Age (years) (mean = 53.4)
<18 28 8.1
18 to <50 97 28
50+ 221 64
Sex
Male 153 44
Female 193 56
Race and ethnicity
†
White, non-Hispanic 239 71
non-White or Hispanic 99 29
Adults only
Years lived at current address (mean = 20.8)
<10 80 25
10 to <20 82 26
20 to <30 77 24
30+ 79 25
Current primary drinking water source
Public water system 217 68
Bottled water 101 32
Average tap water consumption while living at current home (8-
ounce cups per day)
(mean = 6.4)
0 45 14
>0 to <2 13 4.1
2 to <4 40 13
4 to <6 60 19
6 to <8 44 14
8+ 114 36
Current use of treatment or filtration device
One or more filter/treatment device(s) 190 60
None 128 40
Occupational exposures to PFAS in the past 20 Years
One or more occupational exposure(s) 41 13
None 227 87
* The sums of participants for different fields in this table do not always add up to expected values, because not
every participant answered corresponding questions during the questionnaire.
†
ATSDR collapsed categories for race and ethnicity for all analyses because of the few responses across
categories.
‡
The sums of percentages for different fields in this table do not always add up to 100%, because not every
participant answered corresponding questions during the questionnaire and because of rounding

15
The average age of EA participants was 53.4 years, and 71% of the participants identified themselves as
White, non-Hispanic. Of EA participants, 56% identified as female, 44% identified as male, and 92% were
adults, aged 18 years or older. The age cutoff is important because adults were administered a different
exposure history questionnaire with more detailed questions. Among the adult participants, 75%
reported living in their current homes for more than 10 years.
Adults were also asked about their current primary source of drinking water: 68% said public water
system (Security WD, Widefield WSD, or Security MHP), and 32% said bottled water. Adults reported
drinking an average of 6.4 8-ounce cups of water a day at home, and 60% said they currently use some
type of filtering or treatment device for their drinking water. Examples include filters on refrigerators,
pitchers, and faucets; whole-house carbon filtration systems; and reverse osmosis treatment systems.
The questionnaire asked adults for their occupational histories over the past 20 years; 13% reported
holding one or more jobs with potential PFAS exposures (e.g., firefighting, military, aviation).
Comparison of Security-Widefield EA Participants’ Demographics to Sampling
Frame Demographics
This EA was designed to estimate PFAS levels in blood that were generalizable to the sampling frame as
a whole (i.e., Security-Widefield households in the affected area shown in Figure 1). The recruitment
method used for this EA ensures the absence of selection bias—that is, everyone in the sampling frame
had an equal chance of being chosen to participate. However, ATSDR also explored the potential for
participation bias—that is, substantive differences between those who chose to participate and those
who did not.
ATSDR used 2010 Census data (Table 4) [USCB 2010] to compare the EA participants’ demographic
profile with the profile of all residents in the sampling frame. The comparison revealed the following:
• Age distribution. The EA participants included a higher proportion of older adults (age 50+
years), a lower proportion of younger adults (18–50 years), and a lower proportion of children
(age <18 years) than the sampling frame population (Table 4). Specifically, 64% of the EA
participants reported being 50 or older, but 29% of the sampling frame population falls in this
age range (ATSDR chose 50 years as a cutoff for older and younger adults based on the median
age of menopause in the United States, which may affect exposure profiles). Similarly, 28% of
the EA participants reported being 18–50, but 43% of the sampling frame population falls in that
age range. Finally, 8.1% of the EA participants reported being <18 years, but 28% of the
sampling frame population falls in that age range.
• Race/ethnicity. Among the race/ethnicity characteristics, only the percent of residents who
identify as White and more than one race showed a significant difference between the EA
participants and the sampling frame population (Table 4). Specifically, the EA population had
statistically more White participants (79%) than the sampling frame population (74%) and fewer
participants who identified as more than one race (3.5%) than the sampling frame (8.3%). For
this comparison, combined race and ethnicity were not available at the block level from the
Census. Therefore, only ethnicity and the race categories of White, Black, and More than one
race were compared because of the small number of respondents in other categories.
The effect of age on blood levels and its implications on community statistics is further explored
throughout this report. Refer to the “Discussion” section for ATSDR’s assessment of how these
demographic differences influence data interpretations.
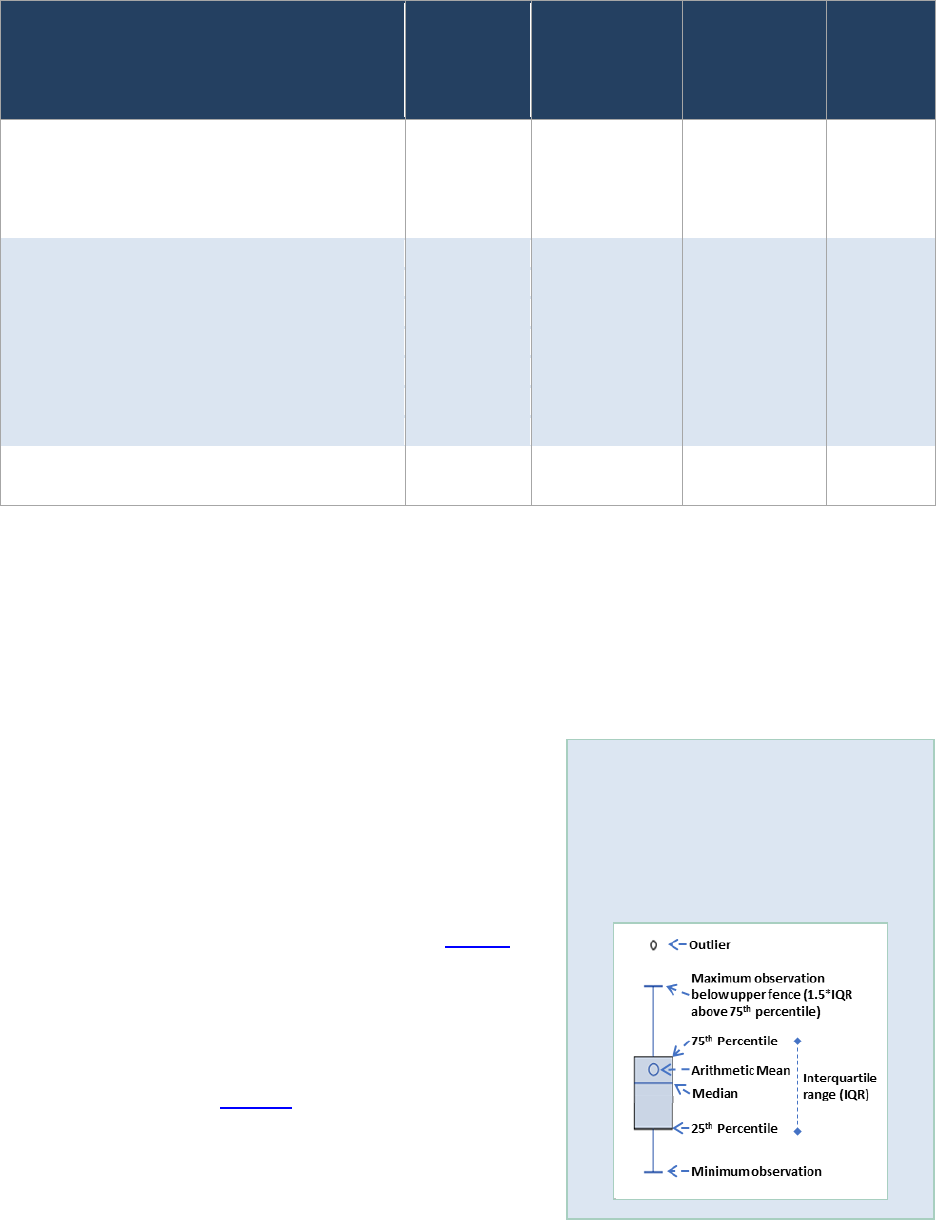
16
Table 4. Demographic comparison of EA participants and the sampling frame population
Demographics
Number of
Participants
(n)*
Percent of
Participants
(%)
Sampling
Frame
Distribution
(%)
†
p-Value
‡
Age Group (years)
<18 28 8.1 28.1 <0.001
18–50 97 28.0 43.2 <0.001
50+ 221 63.9 28.7 <0.001
Race
White 275 79.5 73.7 0.017
Black or African American 28 8.1 9.2 0.52
Am. Indian & AK Native <10 — 1.1 —
Asian <10 — 2.8 —
Nat. Hawaiian/Pacific Islander <10 — 0.88 —
More than one race 12 3.5 8.3 0.0016
Ethnicity
Hispanic or Latino (of any race) 57 16.5 18.5 0.38
*
Counts may not sum to total because participants may have refused to answer questions. Counts are not shown
for categories with fewer than 10 participants.
†
Sampling frame data are based on the 2010 U.S. Census. Demographic characteristics of the sampling frame
may have changed between 2010 and 2020, the time of this EA.
‡
Two-sample test for equality of proportions with continuity correction comparing EA and 2010 Census data. A p-
value of less than 0.05 indicates a statistically significant difference between EA participants and all residents in
the sampling frame.
PFAS in Blood
This section summarizes PFAS levels that ATSDR measured
from the 346 blood samples provided by eligible participants.
Results are summarized in tables and ‘box and whisker’ plots
(see text box).
Unadjusted Community Statistics for PFAS in Blood
ATSDR first calculated the geometric mean levels of PFAS
without accounting for the possible effect of age. Table 5
summarizes results for the seven PFAS measured in Security-
Widefield EA participants’ blood for all ages. Six of the seven
PFAS—PFHxS, PFOS, PFOA, PFNA, PFDA, and MeFOSAA—
were detected in more than 67% of the blood samples.
ATSDR’s statistical analyses throughout this section focus on
these six chemicals, and
Figure 2 shows the distributions of
the individual measurements on a log
10
scale. The log
10
scale
allows for more easily visualizing the wide range of serum
concentrations as it uses equal spacing for each factor of 10
increase. The PFAS found at highest levels were PFHxS
How to read a box and whisker plot:
A box and whisker plot illustrates a
summary of the data using different
statistical measures. See the image
below for how to interpret the
figures throughout this report.

17
(geometric mean = 10.6 micrograms per liter (or µg/L)), PFOS (6.22 µg/L), and PFOA (2.14 µg/L).
One PFAS—PFUnA—was detected in fewer than 60% of the samples. Low frequency of detection for
PFUnA is consistent with NHANES data. Detailed statistics are not included for this chemical, and
concentration percentiles (25
th
, 50
th
, 75
th
, 90
th
, 95
th
) are shown only for measurements above the LOD.
The precision of geometric mean estimates for this EA for all PFAS ranged from 0.2% to 16% depending
on the PFAS (Appendix B, Table B2). Except for Sm-PFOS, these values are all below the desired precision
of 15% used to determine the target sample size for this EA. The collected data met the precision target
specified in the EA protocol.
Table 5. Community statistics for PFAS in blood in micrograms per liter
PFAS
FOD
(%)
Max
Geometric
Mean
95% CI for
Geometric
Mean
Percentiles
25
th
50
th
(Median)
75
th
90
th
95
th
PFHxS 100 138.2 10.6 9.19–12.3 4.93 11.6 24.4 43.2 55.9
PFOS NA* 42.5 6.22 5.53–6.99 3.65 6.50 11.5 18.1 23.8
PFOA NA* 16.8 2.14 1.96–2.34 1.28 2.18 3.45 5.25 6.41
PFNA 95.1 2.4 0.286 0.262–0.312 0.135 0.243 0.390 0.680 0.845
PFDA 68.5 0.9 0.123 0.113–0.133 NA
†
NA
†
0.138 0.241 0.361
PFUnA 41.3 1.6 NA
‡
NA
‡
NA
†
NA
†
NA
†
0.138 0.183
MeFOSAA 67.1 2.3 0.134 0.121–0.148 NA
†
NA
†
0.169 0.293 0.557
FOD = frequency of detection, CI = confidence interval, NA = not applicable
*
PFOA and PFOS are calculated sums of branched and linear subsets and are not measured directly. Linear PFOA
was detected in 99.4% of samples with a geometric mean of 2.04 micrograms per liter (µg/L); branched PFOA
was detected in 0.3% of samples. Linear PFOS was detected in 99.1% of samples with a geometric mean of 3.98
µg/L; branched PFOS was detected in 99.4% of samples, with a geometric mean of 2.11 µg/L.
†
Percentile is below the LOD.
‡
Per the EA protocol, geometric means were not calculated for PFAS detected in less than 60% of samples.

18
Figure 2. Distribution of PFAS blood levels (log scale)
Community Statistics for PFAS in Blood Age-Adjusted to the Sampling Frame
Since the demographic profile comparison reported above showed that EA participants were
significantly older than the sampling frame as a whole, ATSDR also calculated geometric means that
were age-adjusted to the sampling frame population based on 2010 Census data for comparison. Age-
adjusted geometric means correct for the participation bias discussed earlier and are more generalizable
to the sampling frame community. Table 6
shows that age-adjusted blood geometric means for all PFAS
are lower than unadjusted values. Of the three PFAS with the highest concentration (PFHxS, PFOS, and
PFOA), age-adjusted geometric means are between 20% and 35% lower than unadjusted values. The
lower values for age-adjusted geometric means reported here are consistent with older adults having
higher blood PFAS levels than younger adults. The effect of age and the implications of these age-
adjusted statistics are further discussed throughout this report.
Table 6. Geometric means for PFAS in blood in micrograms per liter, unadjusted and age-
adjusted to the sampling frame
Unadjusted Age-Adjusted to Sampling Frame
PFAS
Geometric
Mean
95% CI for Geometric
Mean
Geometric
Mean
95% CI for
Geometric Mean
PFHxS 10.6 9.19–12.3 6.88 5.70–8.29
PFOS 6.22 5.53–6.99 4.55 3.93–5.26
PFOA 2.14 1.96–2.34 1.72 1.54–1.93
PFNA 0.286 0.262–0.312 0.242 0.222–0.263
PFDA 0.123 0.113–0.133 0.118 0.108–0.130
PFUnA
NA
*
NA
‡
NA
*
NA
*
MeFOSAA 0.134 0.121–0.148 0.112 0.101–0.124
CI = confidence interval, NA = not applicable
* Per the EA protocol, ATSDR did not calculate geometric means for PFAS detected in less than 60% of samples.

19
Comparison of EA Participants’ PFAS Blood Levels to the National Population
This section compares PFAS levels among Security-Widefield EA participants to levels found in the U.S.
general population. To explore effects related to differences in the age distribution of EA participants vs.
the NHANES population, ATSDR calculated both unadjusted geometric means of all EA participants and
geometric means adjusted to the age distribution of the U.S. population in NHANES 2015–2016.
Table 7
shows the unadjusted comparison for the entire pool of EA participants to the data available
from NHANES, which are the geometric means for the 2015–2016 survey [CDC 2019]. For PFHxS, PFOS,
PFOA, unadjusted geometric mean blood levels among Security-Widefield EA participants were
statistically (p<0.05) higher than the national geometric mean. For PFNA and PFDA, the unadjusted
blood levels among Security-Widefield EA participants were statistically lower than the national
geometric mean. Per protocol, geometric means were not calculated during NHANES for PFAS detected
in less than 60% of samples, which included MeFOSAA. In this EA, MeFOSAA was detected in more than
60% of samples and geometric means were calculated.
Of the PFAS analyzed in blood, PFHxS levels had the largest elevations when compared to national
levels. The unadjusted geometric mean blood PFHxS level among Security-Widefield EA participants was
9.0 times the national level. Blood PFHxS levels were above the national geometric mean for 96% of EA
participants and above the NHANES 95
th
percentile for 75% of EA participants (Table 7). The unadjusted
geometric mean blood PFOS level among Security-Widefield EA participants was 1.3 times the national
level. Blood PFOS levels were above the national geometric mean for 65% of EA participants and above
the NHANES 95
th
percentile for 9.8% of EA participants. The unadjusted geometric mean blood PFOA
level among Security-Widefield EA participants was 1.4 times the national level. Blood PFOA levels were
above the national geometric mean for 69% of EA participants and above the NHANES 95
th
percentile for
19%.
On average, total PFOS measurements were composed of 65% linear PFOS (n-PFOS) and 35% branched
PFOS (Sm-PFOS). The proportion of n-PFOS found in EA participants’ blood is lower than that found in
standard PFOS products (76%–79%)
[Kärrman et al. 2007] but comparable to levels found in the blood of
the general U.S. population [CDC 2019]. Measurements of total PFOA were composed of 97% linear
PFOA (n-PFOA) and 3% branched PFOA (Sb-PFOA), which is also comparable to the proportions found in
the U.S. population [CDC 2019]. All remaining statistical analyses in this report focus on total PFOA and
total PFOS rather than treating the linear and branched isomers separately.
For this EA, ATSDR also calculated geometric means age-adjusted to the NHANES population. Because
the 2015–2016 NHANES survey does not report data for individuals under 12 years of age, these
geometric mean calculations are based on the 337 EA participants. Table 7 and Figure 3
show blood
PFAS geometric means adjusted to the NHANES population differ from unadjusted values. The adjusted
geometric mean blood PFHxS level among Security-Widefield EA participants was 6.8 times the national
level. The age-adjusted geometric mean blood PFOA level among Security-Widefield EA participants was
1.2 times the national level. Even when controlling for the age-distribution in the population, EA
participants had statistically higher blood levels of PFHxS and PFOA than the U.S. population. After
adjusting for age, blood levels of PFOS in EA participants were higher than the U.S. population, but the
difference was not statistically significant.

20
Table 7. Comparison of PFAS blood geometric means (GMs) and 95th percentiles in Security-
Widefield, Colorado, with the U.S. population (NHANES 2015–2016) in micrograms per liter
PFAS
NHANES GM
(CI)*
Security-
Widefield GM
(CI)
†
:
Unadjusted
Security-
Widefield GM
(CI)
†
: Age-
Adjusted to
NHANES 2015-
2016
Percent of
Security-
Widefield
Results
over
NHANES
GM (%)
NHANES
95
th
Percentile*
Security-
Widefield
95
th
Percentile
Percent of
Security-
Widefield
Results over
NHANES 95
th
Percentile (%)
PFHxS
1.18
(1.08–1.30)
10.6
(9.19–12.3)
p<0.001
8.08
(6.88–9.50)
p<0.001
96.0 4.90 55.9 75.1
PFOS
4.72
(4.40–5.07)
6.22
(5.53–6.99)
p<0.001
5.15
(4.48–5.91)
p=0.27
65.3 18.3 23.8 9.83
PFOA
1.56
(1.47–1.66)
2.14
(1.96–2.34)
p<0.001
1.82
(1.65–2.02)
p=0.009
68.5 4.17 6.41 18.8
PFNA
0.577
(0.535–0.623)
0.286
(0.262–0.312)
p<0.001
0.245
(0.223–0.270)
p<0.001
18.2 1.90 0.845 0.290
PFDA
0.154
(0.140–0.169)
0.123
(0.113–0.133)
p<0.001
0.119
(0.1.08–0.131)
p<0.001
33.0 0.700 0.361 1.16
PFUnA NA
‡
NA
‡
NA
‡
NA 0.400 0.183 1.45
MeFOSAA NA
‡
0.134
(0.121–0.148)
§
0.122
(0.110–0.136)
§
NA 0.600 0.556 4.62
CI = 95% confidence interval, NA = not applicable
*
Source: CDC 2019
†
P-values represent a t-test comparison between Security-Widefield GM and NHANES GM.
‡
Per the protocol, geometric means were not calculated for PFAS detected in less than 60% of samples.
§
No statistical comparison could be made with NHANES because NHANES did not calculate a geometric mean for
this PFAS because this PFAS was detected in less than 60% of NHANES samples.

21
Figure 3. EA average PFAS blood levels compared to national levels
Correlations Among PFAS in Blood
ATSDR also evaluated correlations between PFAS in blood (log
10
). This analysis determined whether any
PFAS tended to have similar patterns in the blood of Security-Widefield EA participants. ATSDR used
Pearson correlation coefficients (r) for this analysis. An r of 0 means two data sets are uncorrelated, and
an r of 1 means two data sets are exactly correlated (i.e., they rise and fall in proportional amounts). The
higher the coefficient, the closer the correlation. Table 8
shows the Pearson correlation coefficients for
the five most frequently detected PFAS.
PFHxS, PFOS, and PFOA blood levels showed the strongest correlations (Table 8). All pairings of these
chemicals had Pearson correlation coefficients relatively close to 1 (r = 0.71–0.73). On the other hand,
PFNA and PFDA were correlated with each other (r = 0.68) and had weak to moderate correlations with
other compounds (r = 0.13-0.61). MeFOSAA had weak or no correlations with all other compounds (r=-
0.038-0.29).
Table 8. Pearson correlation coefficients between PFAS in blood (log)
PFHxS PFOS PFOA PFNA PFDA MeFOSAA
PFHxS 1.00 0.72 0.73 0.32 0.13 0.22
PFOS 0.72 1.00 0.71 0.61 0.41 0.29
PFOA 0.73 0.71 1.00 0.57 0.35 0.19
PFNA 0.32 0.61 0.57 1.00 0.68 0.19
PFDA 0.13 0.41 0.35 0.68 1.00 -0.038*
MeFOSAA 0.22 0.29 0.19 0.19 -0.038* 1.00
* Correlations not significant, i.e., p>0.05.

22
PFAS Blood Levels by Demographics and Other Exposure Characteristics
This section examines how the demographic and exposure history information collected during the
questionnaire relates to blood PFAS levels. Since different questionnaires were administered to adult
and child participants, responses were analyzed separately. Additionally, some questions were
applicable only to female adult participants and are therefore also presented separately. Appendix C
(Tables C1 and C2) summarizes all adult and child questionnaire responses.
ATSDR used univariate and multivariate models to
evaluate the relationships between questionnaire data
and blood PFAS levels. This section summarizes
relationships that were found to be statistically
significant. For this EA, the following demographic and
exposure characteristics had an association with at
least one PFAS in either univariate or multivariate
models:
• age,
• sex,
• tap water consumption,
• drinking water source,
• use of a water filtration or treatment device,
• drinking water consumption rate,
• length of residence in the sampling frame,
• public water supply,
• kidney disease history,
• occupational exposure,
• consumption of selected local food items,
• cleaning frequency,
• breastfeeding (adult females and children), and
• childbirth (adult females).
Table 9 summarizes the demographic and exposure characteristics that were statistically significant in
each adult multivariate model.
ATSDR created mathematical models
to identify demographic and lifestyle
characteristics associated with PFAS
blood levels.
Univariate models evaluated the
effects of one variable, or exposure
characteristic, at a time while
multivariable models evaluated the
joint effect of multiple characteristics
on blood PFAS levels at the same time.
Multivariable regression models
describe the average increases in PFAS
blood levels for each unit increase in
the exposure characteristics.

23
Table 9. Summary of statistically significant variables (p<0.05) in multivariate regression
models
Parameter
PFHxS PFOS PFOA
All
Adult
Adult
Female
Adult
Male
All
Adult
Adult
Female
Adult
Male
All
Adult
Adult
Female
Adult
Male
Age (continuous)
—
Sex (categorical)
NA NA
NA NA — NA NA
Age × sex (continuous)*
NA NA — NA NA — NA NA
Years in sampling frame in the
past 20 years (continuous)
—
—
Kidney disease history
(categorical)
—
— — — — — —
Occupational Exposure
(categorical)
—
— — — — — —
Filter use (categorical) — — — —
Consumption of fruits and
vegetables (categorical)
— — —
—
— — —
Home cleaning frequency
(categorical)
— — — — — — —
= statistically significant, ‘—’ = not statistically significant, NA = not applicable
* This variable is an interaction term between age and sex.
The following subsections briefly summarize results for these topics. All other results are presented in
Appendix C, as described below.
• Tables C1 and C2 present response
frequencies for all questions included in the
adult and child questionnaire, respectively.
These tables also present geometric means
and 95% confidence intervals around
geometric means stratified by the response
options (e.g., statistics are presented
separately for males and females) for PFHxS,
PFOS, PFOA, PFNA, PFDA, and MeFOSAA.
While blood levels of PFNA, PFDA, and
MeFOSAA were not found to be statistically
higher than the national geometric means,
both PFAS were detected at a high enough
frequency (greater than 60%) to present
meaningful results. Summary statistics are
therefore provided in Appendix C for
completeness, but not discussed below.
• Tables C3 and C4 present univariate
modeling results for all questions in the adult
and child questionnaire for the same six
PFAS, as data allow. Data are presented only
Goodness of Fit Measure
R-squared or R
2
is a statistical measure used
to evaluate how well a mathematical model
explains the measured data by looking at the
differences between the observed PFAS
concentrations and values predicted by the
model.
• An R
2
of 1 means the model completely
predicts the observed PFAS
concentrations, so that there are no
differences between the model and the
PFAS concentrations and 100% of the
PFAS concentrations are explained by the
model.
• An R
2
of less than 1 means that there are
measurements scattered higher and/or
lower than the model predictions and
there are differences
between the two.

24
when a category had at least 10 responses. Some categories were collapsed to meet this
threshold.
• Tables C5–C12 present multivariate modeling results for PFHxS, PFOS, and PFOA. Multivariate
models, including the goodness-of-fit measure, R-squared or R
2
, are presented separately for all
adults, male adults only, and female adults only. The closer the R
2
value is to 1, the more the
variables in the model explain the variability in blood PFAS levels. Across all models, R
2
values
ranged from 0.13 to 0.30. ATSDR modeled males and female adults separately to explore sex-
specific differences including the potential effect of childbirth and breastfeeding on female
blood PFAS levels. The variables considered in male-only and female-only models were limited
to those that were significant in final all-adult models. Final multivariate male-only models were
only significant for PFHxS and PFOA; the best model for PFOS was a univariate model consisting
of only a single significant variable. The final female-only models were only significant for PFHxS
and PFOS. ATSDR did not develop multivariate models for children because of the small sample
size for this population (n=28).
• Figures C1–C36 present box and whisker plots for unadjusted blood levels by each demographic
and exposure characteristic included in the statistical analyses.
Blood PFAS Levels and Age
Because many studies have found that older people have
higher blood PFAS levels, ATSDR investigated how Security-
Widefield EA participants’ ages related to their blood levels.
As Figure 4
illustrates, the blood levels for PFHxS, PFOS, and
PFOA increased with age in adults, but trends were
inconsistent in children.
For adults, ATSDR’s univariate analysis showed that blood
PFHxS, PFOS, and PFOA were higher in older individuals than
in younger individuals, and this finding was statistically
significant. As Figure 4 shows, PFHxS had the strongest age
dependence. The univariate analysis indicates that on
average, blood PFHxS levels in Security-Widefield EA
participants increased 2.5% for every year of participant age
in adults. This suggests a 28% increase in blood PFHxS levels
for every 10 years of participant age in adult participants.
The calculated age-related increases for PFOS (1.9% per year
of participant age) and PFOA (1.3% per year of participant
age) were lower.
ATSDR’s multivariate analysis provided further perspective on this trend, showing that the age
dependence was generally stronger for women than men among adults for PFHxS. For example, the all-
adult model for PFHxS (Appendix C, Table C5) suggests a 2.5% increase in blood PFHxS for every
additional year of participant age in female participants, and a 1.3% increase in blood PFHxS levels for
every additional year of participant age in males, when controlling for other characteristics; these
findings were statistically significant. Similar results were observed in the stratified male-only and
female-only models. Age also remained a significant predictor of blood levels for PFOS (1.7% per year)
and PFOA (1.0% per year) in all-adult multivariate models.
Variability describes the spread or
dispersion of data values. If the values
are similar to each other there is little
variability, if the values are spread out
there is more variability.
Multivariable regression can help us
understand how much of the
variability in PFAS blood levels can be
explained by the combination of
factors in the model such as age, sex,
and length of residency among others.
If the model does not explain a large
portion of the variability, that means
there are other unknown factors
influencing PFAS levels in blood.

25
Age was not statistically associated with blood PFAS levels in children under 18 in univariate analyses.
Note that multivariate models were not explored for children because of the small sample size.
Figure 4. PFAS blood levels in adults and children (log scale)
Blood PFAS Levels by Sex
ATSDR investigated how blood PFAS levels vary between males and females because previous research
has shown that, all other factors considered equal, adult males tend to have higher blood PFAS levels
than adult females. ATSDR’s univariate analyses showed that PFAS levels were higher in adult males
than in adult females for PFOS. Modeled blood levels in adult males were 43% higher for PFOS (
Figure
5). This estimate for PFOS was similar when controlling for other variables in multivariate models (42%).
When controlling for other variables, sex was also a significant predictor of blood PFHxS levels, and the
difference between males and females was larger in younger people. For example, 30-year-old males
had higher modeled blood PFHxS levels than 30-year-old females by 70%. For 50-year-old males, this
difference was reduced to 35% compared to 50-year-old females.
Blood levels of these three PFAS were not statistically associated with sex in children.

26
Figure 5. PFAS blood level in adults by sex (log scale)
Blood PFAS Levels and Tap Water Consumption
ATSDR investigated several questions from the adult and child questionnaires to characterize
relationships between blood PFAS levels and consumption of PFAS-contaminated drinking water. These
questions are about the drinking water source, amount of tap water consumed at home or school, and
residential history. In some cases, data trends may have been affected by subtleties in the wording of
exposure history questions, as described below. ATSDR also considered the effect of each participant’s
public drinking water system.
Drinking water source. For adults, ATSDR first considered participants’ primary drinking water source.
Adult participants were asked, “What is your current main source of drinking water in your home?” All
of the responses were tap water (68%) or bottled water (32%). In univariate analyses, adults who
primarily drank bottled water had significantly lower PFHxS (31%) blood levels when compared to adults
who primarily drank from a public water system. (Figure 6
). However, when controlling for other
variables in multivariate analyses, this association did not remain statistically significant. Note that the
exposure history question asked about current drinking water sources. It is possible that some
participants who reported currently drinking bottled water previously drank tap water when their
drinking water was contaminated.

27
Figure 6. PFAS blood level in adults by drinking water source (log scale)
Use of filtration device. ATSDR also considered relationships between blood PFAS levels and current use
of drinking water filtering and water treatment devices. As Figure 7 shows, 60% of participants reported
using a filter or treatment device on the tap water that they drink at home, 26% of participants reported
no filter or treatment device on the tap water that they drink at home, and 14% reported not drinking
tap water at all. In ATSDR’s univariate analyses, participants who reported not drinking tap water at all
had significantly lower PFHxS (52%), PFOS (43%), and PFOA (32%) blood levels when compared to those
who drank tap water with no treatment of filter device. When controlling for other variables in
multivariate analyses, not drinking tap water remained statistically significant in the all-adult
multivariate models with lower concentrations for PFHxS (36%), PFOS (32%), and PFOA (24%). This
association also remained statistically significant in the PFHxS and PFOS female-only multivariate
models.

28
Figure 7. PFAS blood level in adults by filter type (log scale)
Consumption rates. ATSDR also considered
participants’ self-reported tap water consumption
rates (Figure 8
). Adult participants were asked,
“During the time you lived in a home served by the
water source identified above [i.e., for the question
quoted three paragraphs ago], on average how many
8-ounce cups of water or beverages prepared with
tap water did you drink while at home per day?” In
univariate analyses, for every additional cup of tap
water an adult reported drinking at home per day,
blood PFHxS, PFOS, and PFOA increased by 3.7%,
2.0%, and 1.7%, respectively. However, these
associations did not remain significant in multivariate
analyses, which controlled for other potential
confounders.
As can be seen in Figure 8, 8% of participants
reported consumption rates that fall above the higher
end values (95th percentile) reported in EPA’s
Exposure Factors Handbook of 3,292 milliliters per
day (approximately 14 cups) [EPA 2019]. This
relatively small percentage of participants may have
overestimated their drinking water consumption, but
this is not expected to alter conclusions.
What are confounders?
Confounding is a distortion in the
estimated relationship between a
potential predictor and measure of
exposure due to the presence of a third
variable—called a confounder. In order for
confounding to occur, that third variable
must be associated with both the
predictor (or independent variable) and
the measure of exposure (or dependent
variable). For example, age can act as a
confounder on the estimated strength of
association between length of residence in
the sampling frame and blood PFAS levels.
By adjusting for these types of
confounding variables in multivariate
statistical models, ATSDR can calculate
less biased estimates of the relationships
between dependent and independent
variables of interest.

29
Figure 8. PFAS blood level in adults by tap water consumption rates (log scale)
Length of residency. For adults, ATSDR also considered the length of residency. The exposure history
questionnaire asked adults where they had lived for over the past 20 years. ATSDR calculated the total
amount of time participants reported living in the sampling frame over this period. These responses can
serve as a proxy for potential exposure to PFAS-contaminated drinking water in the community. That is,
the longer the residency within the sampling frame, the greater the likelihood of past PFAS exposure
from contaminated drinking water. Any resident reporting prior residences with addresses in Security,
Widefield, or Security-Widefield were assumed to fall within the sampling frame. Any addresses in
question (e.g., addresses in Colorado Springs or Fountain) were mapped and categorized as within or
outside of the sampling frame accordingly.
Figure 9
shows the relationship between reported residence duration in Security-Widefield for the past
20 years and blood PFAS levels. A consistent relationship was observed for PFHxS, PFOS, and PFOA:
blood levels statistically increased with the number of years participants lived in the sampling frame in
the past 20 years for PFHxS (9.8% per year), PFOS (4.1% per year), and PFOA (3.3% per year). The
multivariate analysis showed that all three PFAS continued to have a statistically significant relationship
with residency duration, and this effect was most pronounced for PFHxS. For every additional year that
an adult participant lived in Security-Widefield, blood PFHxS increased by 7.1%, while PFOS and PFOA
increased by 2.0%. This relationship continued to be significant for all PFAS in male-only models and for
PFHxS in female-only models.

30
Figure 9. PFAS blood levels in adults by length of residence in sampling frame (log scale)
Public Water Supply
ATSDR also consider participants’ public water supplies (Figure 10). Participants were asked which public
water supply that were served by. For participants who did not know which public water supply they
were served by, ATSDR mapped their addresses to identify the appropriate public water supply. In the
sampling frame, adult participants generally lived in homes that received drinking water from the
Security WD (n=203) or from Widefield WSD (n=109). One EA participant received water from Security
MHP. In univariate analyses, adult participants connected to Widefield WSD had blood PFOS levels 33%
greater than adult participants connected to Security WD. However, this association did not remain
significant in a multivariate model.

31
Figure 10. PFAS blood level in adults by public water supply (log scale)
Blood PFAS Levels and Kidney Disease
Adult participants were asked about whether they had a history of kidney disease, because it can affect
blood PFAS levels [Barry et al. 2013; Watkins 2013]. The questionnaire results indicated that only 6% of
adults (n=20) reported a diagnosis of kidney disease, but these adults did not have statistically different
blood PFAS levels than those without a diagnosis of kidney disease in univariate analyses. However, in
multivariate analyses, after controlling for other variables, participants who reported a history of kidney
disease had PFHxS blood levels that were 39% lower than those who did not. This variable was also
statistically significant in the male-only multivariate model. The results for kidney disease for this EA are
based on limited data and should be interpreted with caution. Note also that kidney disease was self-
reported and there may be misclassification with this variable.
Blood PFAS Levels and Occupational Exposures
Adult participants were asked about their occupational history over the past 20 years. Participants were
specifically asked about experience working at manufacturers of PFAS or PFAS-containing products (e.g.,
nonstick cookware, water-resistant clothing) and past work in firefighting, the military, or aviation.
Forty-one (13%) adult participants reported at least one occupational exposure in the past 20 years. All
41 participants reported working in either military, aviation, or firefighting. In univariate analyses,
participants with occupational exposures on average had lower blood PFHxS (33%) than adult
participants who reported no occupational exposures in the past 20 years (Figure 11
). In multivariate
models, participants with any occupational exposure continued to have significantly lower blood PFHxS
levels (28%). The direction of this association is the opposite of what was expected, but results are
based on a small number of participants and should be interpreted with caution.

32
Figure 11. PFAS blood level in adults by occupational history (log scale)
Blood PFAS Levels and Consumption of Selected Local Food Items
Some PFAS accumulate in plants, fish, and animals. The questionnaire asked adult and child EA
participants how often they consume locally grown fruits and vegetables, locally caught fish, and milk
from animals in the sampling frame. Too few adult EA participants reported consuming locally produced
milk (n=5) to allow for meaningful statistical analyses, and a statistically significant relationship was not
observed between consumption of locally caught fish and blood PFAS levels, though only 11 adults
reported consuming locally caught fish.
Blood PFAS levels were not associated with consumption of locally grown fruits and vegetables in
univariate analyses. However, in multivariate analyses, blood PFOS levels were higher by 52% among
adult EA participants who reported any consumption of locally grown fruits or vegetables (n=161)
compared to participants who reported no such consumption (n=154). Note that sex-specific models
showed that this relationship was primarily observed in males. While levels of PFOS were higher in
participants who consumed local produce, PFOS blood levels were not elevated in the community.
Blood PFAS Levels and Cleaning Fequency
Adult participants were asked about the frequency at which they clean their homes. In univariate
models, adult participants who reported cleaning their homes three times per week or more on average
did not have statistically different blood PFAS levels than adult participants who reported cleaning their
homes a few times per month or less. However, in all adult multivariate models, adult participants that
reported cleaning their homes three times per week or more on average had PFOS blood levels 24%
higher than adult participants that reported cleaning their homes a few times per month or less. Sex-
specific models showed that this relationship was primarily observed in females. While levels of PFOS
were higher in participants who cleaned their homes more frequently, the community’s average PFOS
blood level was not elevated.

33
Blood PFAS Levels and Past PFAS Blood Levels
Adult participants were asked if they previously had their blood tested for PFAS. Four EA participants
from three households submitted blood PFAS test results from the PFAS Assessment of Water and
Resident Exposure (PFAS-AWARE) health study, which tested PFAS levels in approximately 200 people in
El Paso County in 2018. Approximately 50 participants were retested in 2019 as part of the PFAS-AWARE
study. Information can be found online at https://pfas-aware.org
. Two additional participants from one
household submitted results from independent testing conducted in 2017.
ATSDR compared the change in PFAS blood levels between the first submitted test results for each
participant and the levels measured in this EA. Blood PFHxS and PFOS levels decreased in five of the six
participants between 8.0% and 13% per year and between 7.7% and 20% per year, respectively. In one
participant, PFHxS increased by 11% per year and in a different participant PFOS increased by 13% per
year. In all six participants, blood PFOA levels decreased by between 0.3% and 19% per year.
Blood PFAS Levels and Breastfeeding
During breastfeeding, some PFAS in the breast milk might be transferred from mother to child
Therefore, breastfeeding might reduce PFAS levels in mothers and increase PFAS levels in their
breastfed children [Kim 2020; Kingsley 2018]. Accordingly, the adult and child exposure history
questionnaires included questions about breastfeeding. A question was also included for children about
their consumption of formula (as opposed to breast milk), and if the formula was made using tap water.
Among adult female EA participants, 52% reported that they had breastfed a child, with an average
breastfeeding duration across all pregnancies of 17 months. In univariate and multivariate models for
adult females, neither having ever breastfed a child (yes/no) nor breastfeeding duration was associated
with PFAS serum levels.
Among child EA participants, ATSDR was unable to evaluate the association between having been
breastfed (yes/no) and blood PFAS levels because of the small sample. However, in univariate models
for children, the longer a child breastfed, the greater their blood levels of PFOS and PFOA. Each month
of reported breastfeeding was associated with an increase of 2.4% in blood PFOS and 2.2% in blood
PFOA. For example, 6 months of breastfeeding was associated with an infant’s modeled PFOS blood
level increasing from 2 µg/L to 2.3 µg/L.
Approximately one-third of the children in the Security-Widefield EA (36%) consumed infant formula
reconstituted with tap water (some of these children were also breastfed). In univariate models,
children that reported ever drinking formula reconstituted with tap water on average had blood PFHxS,
PFOS, and PFOA levels that were 57%, 44%, and 40% lower than children that reported never drinking
formula reconstituted with tap water. Similarly, each month of formula consumption was associated
with a decrease of 3% for blood PFOA.
Blood PFAS Levels and Childbirth (adult females and children)
The adult questionnaire asked female participants whether they had any biological children, and if so,
how many. Most adult female EA participants (84%) reported having biological children. Adult female
participants who reported having children on average had blood PFHxS levels that were 45% greater
than adult female participants who reported having no children. Similarly, each child was associated
with 17% increased PFHxS blood levels and 11% increased PFOS levels in univariate models. However,
these relationships were not significant in multivariate models.
34
Blood PFAS Levels and Other Variables
Through the exposure history questionnaires, ATSDR gathered information on several other possible
contributing factors to PFAS exposures. The variables listed below were not statistically associated with
blood levels of PFHxS, PFOA, and PFOS among EA study participants in univariate or multivariate
analyses. In some cases, ATSDR was not able to assess particular relationships because of small number
of participant responses.
• Race/Ethnicity. Adult and child participants were asked to provide information about their race
and ethnicity. However, because there were not enough participants in different race and
ethnicity categories to support robust statistical analyses, ATSDR focused on differences
between Security-Widefield EA participants who self-identified as White, non-Hispanic and
those who identified as non-White, or Hispanic. No statistical relationship was observed for self-
reported race/ethnicity and blood PFAS level in adults.
• Blood donation frequency. Adult participants were asked how often they donate blood or
plasma, because frequent blood and plasma donations might result in decreasing blood PFAS
levels. Relatively few participants (n=12) reported donating blood once or more a year, and no
statistically significant relationship was observed with blood PFAS levels in adults.
• Stain-resistant product use. Many stain-resistant products used to treat fabrics and carpet have
been formulated with PFAS. The exposure history questionnaire asked adult participants how
frequently they used these products; such uses may be associated with PFAS exposures.
Security-Widefield EA adult participants with any self-reported stain-resistant product use did
not have statistically elevated blood levels of any PFAS when compared to participants who
reported never using these products.
• Soil exposure. Adult and child participants were asked how often they play in or touch soil or
dirt in the sampling frame. No statistically significant relationship was observed for self-reported
soil contact frequency and blood PFAS levels in adults or children.
• Fast food consumption. PFAS may be present in fast food take-away containers and food
packaging. Consumption of fast food may serve as an additional source of PFAS exposure.
However, among Security-Widefield County EA adult participants, reported frequency of fast
food consumption was not statistically associated with blood PFAS levels. In recent years, fast
food packaging has likely been reformulated to contain shorter chain PFAS. This shift may make
it more challenging to link PFAS exposure to fast food consumption.
• Flooring. Adult participants were asked about the type of flooring in their living rooms, kitchens,
and bedrooms. While carpet has been linked to increased PFAS exposure because PFAS-
containing stain- and grease-repelling coatings are often applied to carpet [Beesoon et al. 2012],
the presence of carpet in EA participants’ rooms was not statistically associated with blood PFAS
levels among adults.
PFAS in Urine
The study protocol calls for ATSDR to initially analyze 10% of urine samples collected. The protocol
indicates that ATSDR will analyze all participants’ urine samples if the initial analysis shows geometric
mean urine concentrations of any PFAS higher than the NHANES 95
th
percentile values; however, this
threshold was not met. Note that only PFBA and PFHxA were detected in more than 5% of the NHANES
samples.
Information on urinary concentrations of PFAS in humans is limited, yet it may be important to
understand exposure to short-chain and alternative PFAS. Because urine is the primary route of

35
excretion for many PFAS, urinary concentrations may reflect more recent exposures than do serum
concentrations. Some PFAS were detected in serum but not in urine. These seemingly contradictory
results highlight the importance of using the appropriate biomonitoring matrix for EA. Concentrations of
biologically persistent compounds (like some PFAS) are expected to be higher in serum than in urine, as
was observed in this assessment. This trend is also evident in other biomonitoring studies in the general
population and in communities with known PFAS exposures [Calafat et al. 2019].
For the Security-Widefield EA, ATSDR randomly selected 36 participants’ urine samples for analysis.
These samples were provided by 34 adults and 2 children, and these individuals lived in 36 different
households. PFBA was the only PFAS detected in any of the 36 urine samples. Of note, the measurement
of trace levels of PFBA faces known challenges, including selectivity of the analytical instrumentation
and potential for external contamination [Abraham et al. 2021]. Therefore, we advise caution when
interpreting the PFBA results.
Table 10
presents PFBA summary statistics for the randomly selected urine samples and national
statistics for comparison. One of the 36 samples had PFBA urine concentrations higher than the NHANES
95
th
percentile. The protocol specified that all urine samples would be analyzed if the geometric mean
exceeded the 95
th
percentile from NHANES. Since no PFAS were detected in more than 60% of the
analyzed samples, no geometric means were calculated for any PFAS in urine and ATSDR did not analyze
the remainder of the urine samples.
Table 10. Community statistics for PFAS in urine reported in micrograms per liter
PFAS
Frequency of
Detection (%)
Range of
Concentrations
(µg/L)
Security-
Widefield
Geometric
Mean
(µg/L)
Security-
Widefield 95
th
Percentile
(µg/L)
NHANES
Geometric
Mean
(µg/L)
NHANES
95
th
Percentile
(µg/L)
PFBA 2.8 ND–0.4 NA* NA** NA* 0.300
µg/L = micrograms per liter, ND = not detected, NA – Not applicable
* Geometric mean was not calculated because chemical was not detected in at least 60% of the samples
(detected in 13.3% of samples in Calafat et al. [2019]).
** 95
th
percentile is below the limit of detection.
PFAS in Tap Water
As noted previously, ATSDR collected tap water samples from 18 randomly selected participant
households and analyzed these samples for PFAS. One household provided two filtered samples, two
households provided only an unfiltered sample, and 15 households provided both filtered and unfiltered
samples. Detection limits were 2 ppt for all PFAS, except for HFPO-DA (5 ppt).
PFAS were detected in three of the 17 filtered samples. In one of the filtered samples, PFBS, PFHxS,
PFHxA, PFOS, and PFOA were detected. In the second sample, PFHxA and PFHpA were detected and in
the third sample, only PFHxA was detected. The maximum concentrations in these filtered samples were
2.1 ppt PFBS, 3.5 ppt PFHxS, 51 ppt PFHxA, 2.3 ppt PFHpA, 11 ppt PFOS, and 3.0 ppt PFOA.
PFHxA was detected in seven of the 17 unfiltered samples. Four of those samples also had a detected
concentration of PFHpA, and one of those samples also had a detected concentration of PFOS. The
maximum concentrations in these unfiltered samples were 57 ppt PFHxA, 2.5 ppt PFHpA, and 3.0 ppt
PFOS.

36
Geometric means were not calculated for any PFAS in filtered or unfiltered tap water because 40% or
more of the results were non-detect. The detection limit, and measured concentrations were below
EPA’s HA of 70 ppt for PFOA and PFOS combined. There are no EPA health advisory levels for PFBS,
PFHxS, PFHxA, or PFHpA.
The reason that a larger number of PFAS were detected in filtered samples is unclear, as one might
assume that filtered water would be less contaminated than unfiltered water. A possible explanation is
related to filter maintenance, though this issue could not be fully explored as part of this assessment.
Because of the limited PFAS detections in the tap water samples, ATSDR did not investigate correlations
between these sampling results and the blood data.
PFAS in Household Dust
ATSDR collected dust samples from the same 18 randomly selected participant households where tap
water samples were collected and analyzed these samples for PFAS. These samples were taken from
multiple locations in each household, including the primary living space as identified by the homeowner
(e.g., living room, family room, television room), the kitchen, and the bedroom in which participants
reported spending the most time. When necessary, additional sampling was performed in other rooms
to allow ATSDR to collect the proper amount of dust for testing.
Table 11
lists the specific PFAS that were measured in dust along with detailed summary statistics (i.e.,
frequency of detection, geometric means, 95% confidence intervals around the geometric means, and
percentiles). Note that several PFAS were not detected in any sample and are therefore not included in
Table 11 (i.e., PFNS, N-EtFOSA, FtS 4:2, HFPO-DA, ADONA, 9CL-PF3ONS, and 11CL-PF3OUdS).
Table 11. Summary statistics for dust samples (n=18) collected in Security-Widefield
PFAS
FOD
(%)
Maximum
Detected
Result (ng/g)
Geometric
Mean
(ng/g)
95% Confidence
Interval for
Geometric Mean
(ng/g)
Percentiles (ng/g)
50
th
(Median)
90
th
95
th
PFBS 72 67.9 3.25 1.56–6.80 2.91 21.9 54.0
PFPeS 11 28.0 NA* NA* 1.05 2.90 5.64
PFHxS 72 267 3.53 1.82–6.86 2.82 9.05 42.2
PFHpS 11 3.25 NA* NA* 0.884 2.88 3.14
PFOS 100 96.0 12.2 7.20–20.7 10.9 48.8 81.5
PFDS 56 9.83 NA* NA* 1.35 5.00 7.63
PFDoS 28 16.3 NA* NA* 1.34 5.13 7.76
PFBA 67 160 11.0 5.76–20.9 7.88 53.2 141
PFPeA 56 10.6 NA* NA* 2.69 6.36 7.12
PFHxA 100 34.2 6.54 4.07–10.5 6.16 24.1 26.4
PFHpA 78 22.2 3.51 1.91–6.44 2.33 16.5 21.7
PFOA 89 65.1 7.99 4.47–14.3 6.52 34.7 39.5
PFNA 94 36.8 6.70 4.04–11.1 5.74 22.9 33.7
PFDA 89 13.4 3.92 2.57–5.97 3.48 11.5 11.8
PFUnA 44 12.2 NA* NA* 1.35 7.79 10.6
PFDoA 56 10.9 NA* NA* 1.88 6.83 8.20

37
PFAS
FOD
(%)
Maximum
Detected
Result (ng/g)
Geometric
Mean
(ng/g)
95% Confidence
Interval for
Geometric Mean
(ng/g)
Percentiles (ng/g)
50
th
(Median)
90
th
95
th
PFTrA 44 5.10 NA* NA* 1.35 3.19 3.57
PFTA 39 8.31 NA* NA* 1.35 3.14 3.69
PFOSA 17 3.13 NA* NA* 1.29 2.45 2.85
N-MeFOSA 6 5.20 NA* NA* 1.20 3.32 3.77
MeFOSAA 61 38.7 2.35 1.33–4.16 1.98 9.66 24.4
N-MeFOSE 61 1,440 26.8 14.0–51.2 19.0 96.1 383
EtFOSAA 72 12.9 3.08 1.92–4.96 2.82 11.1 12.4
N-EtFOSE 17 150 NA* NA* 7.85 21.6 36.1
FtS 6:2 44 54.7 NA* NA* 4.88 42.5 48.5
FtS 8:2 6 12.6 NA* NA* 4.19 9.79 11.4
FOD = frequency of detection, ng/g = nanograms per gram, NA = not applicable
A total of 18 dust samples are summarized in this table.
* Per the EA protocol, geometric means were not calculated for PFAS detected in less than 60% of samples.
Multiple PFAS (PFHxS, PFOS, PFOA, PFBA, PFNA, PFHxA, PFDA, PFHpA, PFBS, EtFOSAA, N-MeFOSE, and
MeFOSAA) were detected in greater than 60% of samples. N-MeFOSE and PFOS were detected with the
highest average concentration. N-MeFOSE and PFOS had geometric mean values of 26.8
nanograms/gram (ng/g)
4
(95% confidence interval = 14.0–51.2 ng/g) and 12.2 ng/g (95% confidence
interval = 7.2–20.7 ng/g). PFHxS and PFOA had geometric mean values of 3.5 nanograms/gram (ng/g)
(95% confidence interval = 1.8–6.9 ng/g) and 8.0 ng/g (95% confidence interval = 4.5–14.3 ng/g),
respectively.
To provide some context to the results summarized above, average levels of PFAS measured in the 18
samples collected as part of this EA were compared to average dust levels reported in other U.S.-based
studies (in communities with or without PFAS contamination). This includes evaluations of indoor dust
collected at 30 homes in the greater Boston area [Fraser et al. 2013], 124 homes in California [Wu 2015],
15 U.S. homes [Karásková et al. 2016], and 19 homes in Minnesota cities with PFAS-contaminated soil
and drinking water [Scher et al. 2018]. Across these studies, PFOA and PFOS were consistently reported
at the highest concentrations. Geometric mean concentrations ranged from 24 to 45 ng/g for PFOA and
27 to 35 ng/g for PFOS [Fraser et al. 2013; Wu et al. 2015]. Two of the studies did not report geometric
means; for these studies, median concentrations were reported at 9 ng/g and 51 ng/g for PFOA and 14
ng/g and 67 ng/g for PFOS [Karásková et al. 2016 and Scher et al. 2018, respectively]. Geometric mean
and median concentrations for PFOA and PFOS measured in the 18 samples collected as part of this EA
were lower than what was reported from these four studies. Details on these studies and comparisons
with all other measured PFAS can be found in Appendix A, Table A1.
While these results suggest that PFOS and PFOA measured in the dust samples collected in Security-
Widefield were found at lower levels than reported elsewhere in the United States, note that the studies
referenced here do not necessarily provide representative comparisons and are provided only for
4
This unit (in this case, representing nanograms of PFAS measured per gram of dust collected) is equivalent to
parts per billion and micrograms per kilogram.

38
additional context. The sample collection methods and analytical methods were also not consistent
among these studies.
ATSDR also evaluated the correlation between PFAS measured in dust and blood. This analysis included
analytical data from 18 dust samples and from the 35 blood samples collected from participants residing
in the same homes. Using log-transformed data, ATSDR calculated Pearson correlation coefficients for
the PFAS measured in at least 60% of the dust and the same PFAS measured blood samples for this
assessment. Data were log-transformed because dust and blood concentrations were log-normally
distributed.
PFOA measured in dust was statistically correlated (r=0.46, p=0.0053) with PFOA measured in blood.
MeFOSAA measured in dust was statistically correlated (r=0.57, p=0.0004) with MeFOSAA measured in
blood. None of the other PFAS measured in dust were statistically correlated (p<0.05) with the same
PFAS measured in blood. Note that the sample size for dust measurements in Security-Widefield is
relatively small. ATSDR will further explore these findings, as well as correlations between different PFAS
measured in dust and blood (e.g., the correlation between PFOA in dust and PFOS in blood) in the report
analyzing data across all EA sites.
The dust results presented here are exploratory and should be interpreted with caution. They are based
on a limited set of samples, and in some cases those samples are based on a small sample mass. The
target sample mass for this study was 1 gram, but this target was not always met. Results based on less
than 1 gram of dust have higher detection limits, a possible source of bias.
Discussion
At least one PFAS was detected in the blood of all Security-Widefield EA participants (100%). Because of
the widespread use of PFAS, such high detection frequencies are common in the general U.S. population
[CDC 2019]. PFHxS, PFOS, PFOA, PFNA, PFDA, and MeFOSAA were the most frequently detected
compounds in Security-Widefield EA participants (detection frequencies above 67%).
Results from this EA were compared to the NHANES data from 2015–2016.
5
Age-adjusted geometric
mean blood levels of PFHxS and PFOA were statistically higher than these national geometric means (6.9
and 1.2 times, respectively), and age-adjusted blood concentrations of PFOS, PFNA, and PFDA were
similar to or lower than national geometric means. ATSDR was unable to compare blood levels of
MeFOSAA because this PFAS was detected in less than 60% of NHANES samples.
All PFAS measured in blood for this EA have been phased out of production in the United States.
Following this phase-out, national blood PFAS levels have been steadily declining since 2000 [CDC 2019].
Differences between geometric mean Security-Widefield EA blood levels, collected in 2020, and the
NHANES 2019-2020 geometric mean (not yet available) could be greater than the differences between
geometric mean Security-Widefield EA blood levels and the NHANES 2015-2016 geometric mean
presented here.
5
Newer NHANES data are now available, but this report (and all individual EA reports) compares EA results to
2015-2016 NHANES data to be consistent with individual results letters provided to participants. ATSDR will
consider including the newer data in the report analyzing data across all EA sites.

39
ATSDR compiled blood PFAS levels for the three most prevalent PFAS (PFHxS, PFOS, and PFOA) to
provide further context on the current (2020) Security-Widefield EA blood levels (Appendix A, Table A2):
• For PFHxS, Security-Widefield EA participants’ blood levels are higher than the national
geometric mean from 1999–2000 (2.1 ppt), the time NHANES first measured PFAS and the time
the highest PFAS levels were observed [CDC 2019]. EA participants blood PFHxS levels are also
higher than levels observed in other communities with contaminated drinking water [PA DOH
2019; ATSDR 2013; Frisbee et al. 2009; NH DHHS 2016; NYDOH 2019].
• For PFOS and PFOA, blood levels among Security-Widefield EA participants are within the range
of those observed in other communities with contaminated drinking water (Appendix A, Table
A2). The levels reported here are lower than the national geometric mean PFOS and PFOA levels
for 1999–2000 (30.4 ppt and 5.2 ppt, respectively) [CDC 2019].
Generalizability of Security-Widefield EA Community Statistics
The random sampling recruitment method used for this EA was designed to produce summary statistics
of blood PFAS levels that were generalizable to the sampling frame as a whole (i.e., Security-Widefield
households in the area shown in Figure 1). Although the population invited to participate was likely
representative of the sampling frame, the population that ultimately enrolled was older. Specifically,
adults aged 50 or older represented 64% of the EA population compared with 29% of the sampling
frame. The EA population and the sampling frame as a whole also statistically differed in the proportion
of people who identify as White and as more than one race. Given the 6.3% response rate, it is also
possible that other factors were present at different rates than the community as a whole.
Since age was associated with blood PFAS levels in univariate analyses, the summary statistics for blood
PFAS (Table 5) may be biased, or deviate from the true value, when generalizing to the entire sampling
frame. ATSDR believes that any bias caused by differences in ethnicity would be minimal because race
and ethnicity were not statistically significant in multivariate analyses for PFHxS, PFOS, and PFOA.
However, ATSDR was concerned about the potential bias caused by the older age of EA participants
since levels of PFAS are known to vary depending on people’s age. Therefore, ATSDR quantified the
magnitude of the bias introduced by age by calculating geometric means that were adjusted to the age
distribution of the sampling frame (
Table 6). This analysis showed that the unadjusted geometric means
for blood PFHxS, PFOS, and PFOA biased high by 20% to 35%. Therefore, the sampling frame age-
adjusted geometric means for PFAS are more representative of the average levels in the community.
Relationships Between Demographics and PFAS Blood Levels
When evaluating differences in demographic factors by PFAS levels, adult males had statistically higher
geometric mean blood levels for PFHxS and PFOS, based on results from the all-adult multivariate
models, but did not have statistically elevated differences for other PFAS. In other studies in
communities with contaminated drinking water and for the general U.S. population [e.g., ATSDR 2013;
NH DPHS 2016; CDC 2019], sex-based differences are likely due to additional excretion routes in females
including through menstrual fluid, breastfeeding, pregnancy, and renal clearance rate differences
[ATSDR 2021]. PFAS have been demonstrated to pass through the placental barrier and into the
developing fetus during gestation, and have been measured in maternal serum, cord blood, breast milk
[Cariou et al. 2015], placenta [Chen et al. 2017], fetal tissue [Mamsen et al. 2019], and neonates [Wang
et al. 2014]. These studies suggest gestation, birth, and breastfeeding as excretion pathways for mothers
and gestation and breastfeeding as potential exposure pathways for infants. In this EA, the effect of
gestation (as measured by the number of children a female reported having had) and the duration of
40
breastfeeding were not significant predictors of PFAS blood levels in adult females. However, in
univariate models of child participants, breastfeeding duration was associated with increased PFOS and
PFOA blood levels, formula consumption (yes/no) was associated with decreased PFHxS, PFOS, and
PFOA blood levels, and formula consumption duration was associated with decreased PFOA blood
levels.
Blood PFAS levels were statistically higher in older adults than younger adults, and the effect of age was
stronger in female participants than males for PFHxS. Blood PFAS levels were found to remain
unchanged with age among children (3–18 years). Differences in the associations between blood PFAS
levels and age in adults and children have been observed in other studies [ATSDR 2013; NH DPHS 2016;
CDC 2019]. Generally, increasing blood levels in adults are due to the long biological half-lives of PFAS
and diminishing excretion rates with increasing age. The half-life of a chemical is the amount of time it
takes for 50% of the substance to be eliminated from the body. Most studies estimate a half-life of
PFHxS between 4.7 and 8.5 years, although some have estimated half-lives as long as 35 years [ATSDR
2021]. Most half-life estimates for PFOS are between 3.3 and 7.4 years, with a maximum of 27 years
[ATSDR 2021]. For PFOA, most studies estimate the half-life between 2.1 and 3.9 years with a maximum
of 10.1 years [ATSDR 2021]. In the presence of continued exposures that exceed clearance rates, PFAS
will accumulate in the human body over time.
In this EA, blood PFAS levels were not associated with age in children under 18. Although this trend was
not statistically significant, in other studies PFAS blood levels and age have been associated with
multiple factors including early life exposures and growth dilution. Early-life exposures may have
occurred since PFAS can cross the placenta and are found in breast milk [ATSDR 2021]. In addition,
hand-to-mouth touching and spending more time closer to the floor with settled dust in toddlers is
much greater than in older children. As a child grows, these early-life exposure factors diminish.
Additionally, large increases in body size lower blood levels despite increasing or constant PFAS body
burdens. This process is known as growth dilution [Koponen et al. 2018].
Significance of Drinking Water Exposures
ATSDR conducted EAs to learn more about how exposure to PFAS-contaminated drinking water affects
blood PFAS levels. This relationship is complicated because EA participants were likely exposed to PFAS
not only in contaminated drinking water but also in various consumer products and food items
unrelated to the water. ATSDR considered the following lines of evidence to understand the potential
significance of the drinking water exposure pathway:
• The two PFAS (PFHxS and PFOA) with statistically elevated blood levels in comparison to
national levels were detected in Security-Widefield’s water supplies as early as 2013. We do not
know if contamination began earlier because no data are available before 2013. The maximum
concentrations observed in finished drinking water in any of the three affected water systems
were 590 ppt for PFHxS, 210 ppt for PFOS, and 90 ppt for PFOA. In 2016, all three water systems
mitigated the contamination; however, these PFAS have very long biological half-lives (on the
order of years). Therefore, even though drinking water PFAS exposures in the Security-Widefield
were significantly reduced in November 2016, past drinking water exposures were likely a
contributing factor to the EA participants’ elevated blood PFAS levels, observed 3 years and 10
months later. Furthermore, in this EA, PFHxS had the largest deviation from the national average
and showed the greatest association with reported drinking water consumption, which is what
would be expected given that PFHxS has the longest half-life of the three PFAS.
41
• PFHxS, PFOS, and PFOA were highly correlated in blood (r between 0.71 and 0.73), suggesting
similar or common background sources or exposure pathways. PFHxS and PFOS, and to a lesser
extent PFOA, have many common exposure sources, as these compounds are often found
together in consumer products. While correlations between PFAS have been observed in other
studies [NH DPHS 2016; ATSDR 2013; CDC 2019], the correlations observed between these three
PFAS in this EA are much higher than those observed in the general U.S. population (r between
0.46 and 0.66) [Calafat et al. 2007b]. Instead, the high correlation between PFHxS, PFOS, and
PFOA is consistent with those found in the blood of people living in communities with
contaminated drinking water [ATSDR 2013], providing further evidence that drinking water was
likely a contributing source of exposure among Security-Widefield EA participants. In addition,
the correlations between PFHxS, PFOS, and PFOA in this study are much higher than the
correlations observed for PFNA, PFDA, and MeFOSAA, three compounds that were detected in
Security-Widefield’s drinking water, providing further evidence of a distinct exposure pathway
for these three compounds.
• Univariate statistical analyses of the EA data found that one of the most consistent predictors of
adult blood PFAS levels was length of residency in Security-Widefield. ATSDR considered
residency duration to be a suitable surrogate for drinking water exposures because only
residents who lived in the sampling frame before November 2016 would have had any exposure
to the PFAS-contaminated drinking water, and because of the likelihood that exposure would
increase with the number of years that EA participants lived in the area. However, since older
adults tended to live in the sampling frame longer, this variable was correlated (r = 0.31) with
age in adults. Because of this, it was unclear from univariate models alone whether the
association between the time someone lived in the sampling frame and PFAS blood levels was
primarily due to age. After controlling for age, sex, and other data characteristics, the
multivariate statistical analysis found that residency duration remained statistically associated
with blood PFHxS, PFOS, and PFOA levels, and tap water consumption did not remain
statistically associated with blood PFAS levels. However, multivariate models conducted
separately for males and females suggest that these relationships were primarily observed in
male participants for PFOS and PFOA. Furthermore, multivariate regression models did not
explain a large portion of the variability in participants’ blood PFAS levels (R
2
ranged between
0.13 and 0.30 in the “all adult” models), indicating that many factors are not accounted for.
• ATSDR investigated several questions from the adult and child questionnaires to characterize
relationships between blood PFAS levels and consumption of PFAS-contaminated drinking
water. In ATSDR’s univariate analysis, increased tap water consumption at home was associated
with increased PFHxS, PFOS, and PFOA. However, these associations did not remain significant
in multivariate models. In ATSDR’s univariate and multivariate analyses, participants who
reported drinking only bottled water on average lower PFHxS, PFOS, and PFOA blood levels than
participants who reported drinking tap water with no filter or treatment device. Even though
drinking water consumption rates were not statistically associated with blood PFAS levels as
expected, the associations with bottled water consumption provided further evidence for a
drinking water exposure route.
• ATSDR also considered which public water system served EA participants. In ATSDR’s univariate
analyses, adult participants connected to Widefield WSD had blood PFOS levels greater than
adult participants connected to Security WD. However, this association did not remain
significant in a multivariate model.
42
Taken together, the data suggest that past drinking water exposure contributed to the elevated blood
levels of PFHxS and PFOA observed in the Security-Widefield EA participants.
Other Exposure Characteristics
Other exposure characteristics that showed significant associations with blood levels of one or more
PFAS in either univariate or multivariate analyses included the following:
• Kidney disease. Previous research shows that kidney disease can affect blood PFAS levels [Barry
et al. 2013; Watkins 2013]. Six percent of adults (n=20) reported a diagnosis of kidney disease,
but these adults did not have statistically different blood PFAS levels than those without a
diagnosis of kidney disease in univariate analyses. However, in multivariate analyses participants
who reported a history of kidney disease had PFHxS blood levels that were 39% lower than does
who did not. The results for kidney disease for this EA are based on limited, self-reported data
and should be interpreted with caution.
• Occupational Exposure. Workers can be exposed to PFAS through job tasks that involve
manufacturing or working with PFAS. In both univariate and multivariate models, adult
participants who reported at least one occupational exposure in the past 20 years on average
had lower blood PFHxS levels that those who reported no occupational exposure. Although this
result was the opposite of expected, it is based on a relatively small sample of participants with
occupational exposure (n=41).
• Local fruits and vegetables. In multivariate analyses, blood PFOS levels were higher among adult
EA participants who reported any consumption of locally grown fruits or vegetables compared
to participants who reported no such consumption.
• Cleaning frequency. In multivariate analyses, adult participants that reported cleaning their
homes three times per week or more on average had higher PFOS blood levels than adult
participants that reported cleaning their homes a few times per month or less.
While these two last exposure characteristics showed significant associations with PFOS, PFOS blood
levels were not elevated in the community. All of these observations are based on limited data and
should be interpreted with caution; they will be re-examined in the report analyzing results across all EA
sites.
Security-Widefield Community-Wide Findings
Finding 1. Average blood levels of PFHxS and PFOA in the Security-Widefield EA site
participants are higher than national levels. Averages of other PFAS were not higher than the
national levels or were detected too infrequently to compare to national levels.
Geometric means (i.e., averages) for PFHxS and PFOA blood levels were statistically higher (p<0.05) in
Security-Widefield EA participants when compared to CDC’s NHANES (2015–2016) testing, which was
limited to people over 12 years old. The statistically higher blood PFAS levels were observed for both
unadjusted geometric means for all EA participants and geometric means adjusted to the age
distribution of the U.S. population from NHANES 2015–2016.
Of the PFAS analyzed in blood, PFHxS had the largest elevations when compared to national levels. The
age-adjusted geometric mean blood PFHxS level among EA participants was 6.8 times the national level.
Blood PFHxS levels were above the national geometric mean for 96% of the Security-Widefield EA
43
participants and above the NHANES 95
th
percentile for 75% of the participants. The age-adjusted
geometric mean blood PFOA level was 1.2 times the national level.
Other PFAS measured in this EA (PFOS, PFNA, PFDA) were not higher than national levels. ATSDR was
unable to compare the geometric mean MeFOSAA levels because MeFOSAA was detected in less than
60% of NHANES samples. PFUnA was detected in fewer than 60% of the EA participant samples; due to
the large percentage of samples below the limit of detection, geometric means were not calculated.
Finding 2. Elevated blood levels of PFHxS and PFOA may be associated with past drinking
water contamination.
PFHxS, PFOS, and PFOA were detected in Security-Widefield water systems as early as 2013, though
contamination likely began earlier. Two of these PFAS (PFHxS and PFOA) had statistically elevated blood
levels compared to national geometric means. The maximum concentrations observed in finished water
in Security-Widefield water systems were 590 ppt for PFHxS, 210 ppt for PFOS, and 90 ppt for PFOA.
By November 2016, actions taken by the three affected water systems reduced PFAS levels in drinking
water below EPA’s HA for PFOS and PFOA. Before 2016, PFAS-containing AFFF were primarily
formulated with PFOS, but also contained various PFAS precursors that could break down in the
environment into other PFAS, such as PFHxS, which could explain the elevated blood PFHxS levels.
PFHxS and PFOA have very long biological half-lives (on the order of years). There were 3 years and 10
months between when the water systems took action to reduce exposure to contaminated drinking
water and collection of biological samples during the EA. Because of the long half-lives of PFHxS and
PFOA, past drinking water exposures may have contributed to the EA participants’ blood levels. PFHxS
has the longest estimated half-life of the three compounds (up to 35 years), which may contribute to
why it exceeded the NHANES 2015-2016 geometric mean by the largest margin.
PFHxS and PFOA were highly correlated in Security-Widefield EA participant’s blood (Pearson correlation
coefficient, r = 0.73). This means that, typically, residents who had elevated blood PFHxS levels also had
elevated blood PFOA levels. This correlation suggests a common exposure source, such as the pre-2017
Security-Widefield public drinking water supplies, though other sources of exposure may also have
contributed to the observed blood levels.
Additional observations from the multivariate analyses support the finding that past exposure to
contaminated drinking water may have contributed to the elevated blood levels.
• First, a consistent and statistically significant predictor of participant blood levels for PFHxS and
PFOA was how long the resident had lived in Security-Widefield during the past 20 years. Each
year of residence in the sampling frame over the past 20 years was associated with a 7.1%
increase in PFHxS levels and a 2.0% increase in PFOA levels.
• Second, adults who reported not drinking tap water at all at home on average had statistically
lower PFHxS (36%) and PFOA (24%) blood levels when compared to those who reported drinking
tap water at home with no filter or treatment device.
Multivariate models conducted separately for males and females suggest differences in the associations
(between blood levels and residency duration/tap water consumption) between males and female
participants.
Taken together, the data suggest that past drinking water exposure contributed to the elevated blood
levels of PFHxS and PFOA observed in the Security-Widefield EA participants.
44
Finding 3. Age, sex, occupational exposure, kidney disease history, local fruit and vegetable
consumption, and home cleaning frequency were associated with some PFAS blood levels.
PFAS blood levels varied with different demographic and exposure characteristics of the participant
population. The following relationships were statistically significant in multivariate analyses in the
Security-Widefield EA data set in adult participants:
• Blood levels of PFHxS, PFOS, and PFOA were higher in older participants, and the size of the
effect varied by sex for PFHxS. In males, blood levels for these compounds increased by 1.0% to
1.7% for every year of participant age. In females, blood levels for these compounds increased
by 1.0% to 2.5% for every year of participant age.
• Males had statistically higher blood levels of PFHxS and PFOS than females. PFOS blood levels in
males were 42% higher than in females. For PFHxS, the difference between males and females
was larger in younger people. For example, 30-year-old males had higher blood PFHxS levels
than 30-year-old females by 70%. For 50-year-old males, this difference was reduced to 35%.
• Adult participants who reported at least one occupational exposure in the past 20 years on
average had lower PFHxS (28%) than adult participants who reported no occupational exposures
in the past 20 years. Although this result was the opposite of expected, it is based on a relatively
small sample of participants with occupational exposure and should be interpreted with caution.
• Adult participants who reported a history of kidney disease had PFHxS blood levels that were
39% lower than those who did not. This result is based on a relatively small sample of
participants self-reporting a history of kidney disease and should be interpreted with caution.
• Adult EA participants who reported any consumption of locally grown fruits or vegetables had
blood PFOS levels that were 52% higher compared to participants who reported no such
consumption. While PFOS levels were higher in participants who reported consuming local
produce compared to those who did not, PFOS blood levels were not elevated in the
community.
• Adult participants who reported cleaning their homes three times per week or more on average
had 24% higher PFOS blood levels than adult participants who reported cleaning their homes a
few times per month or less; however, PFOS blood levels were not elevated in the community.
A few associations were observed in children (<18 years) in univariate analyses, though many variables
could not be examined because of the small number of child participants (n=28). Because of the small
sample size, results should be interpreted with caution. Specifically, the longer a child was breastfed, the
higher blood levels of PFOS and PFOA compared to non-breastfed children, and children that reported
ever drinking formula reconstituted with tap water on average had blood PFHxS, PFOS, and PFOA levels
that were lower than children that reported never drinking formula reconstituted with tap water.
Infants born to mothers exposed to PFAS can be exposed in utero and while breastfeeding. However,
based on current science, the benefits of breastfeeding outweigh the risks for infants exposed to PFAS in
breast milk. The final report on all EA sites will include a more robust analysis of children.
Finding 4. Only one PFAS was detected in urine and at relatively low concentrations.
ATSDR analyzed 36 (10%) of the urine samples collected. Only PFBA was detected; it was detected in
2.8% of the 36 samples that were analyzed. ATSDR did not analyze all participants’ urine samples
because none of the species were detected in more than 60% of the samples analyzed.
45
Finding 5. All Security-Widefield drinking water samples collected during the EA in 2020 met
the EPA’s HA for specific PFAS in drinking water.
This is based on 17 filtered and 17 unfiltered water samples collected in 18 households during the EA.
These results are consistent with recent data collected from the Widefield WSD, Security WD, and
Security MHP water systems.
Finding 6. Patterns and levels of dust contamination measured in participating EA households
are comparable to those reported in selected U.S. studies.
Among the PFAS detected most frequently in household dust samples, N-MeFOSE and PFOS were
measured at the highest average concentrations. No nationally representative comparison values are
available, but geometric mean and median concentrations for PFAS measured in dust collected in the
small subset of participating households (n=18) were within the range of levels reported in a few
published studies of other U.S. communities (with or without known PFAS contamination). Of the PFAS
measured in this EA’s household dust samples, PFOA (r=0.46) and MeFOSAA (r=0.57) were statistically
correlated with the same PFAS measured in participants’ blood. The final report on all EA sites will
include a more robust comparison of PFAS measured in dust and blood.
Limitations
There are several limitations associated with this assessment.
• The random sampling recruitment method used for this EA was designed to measure blood PFAS
concentrations that were generalizable to all Security-Widefield residents who were customers
of the Security WD, Widefield WSD, or Security MHP. However, the EA participant sample may
not be fully representative of the community. Only 6.3% of the households from the random
sample participated in the EA. Participant characteristics were different than those of the area’s
overall population. Participants were older, more likely to identify as White, and less likely to
identify as more than one race. ATSDR addressed some of these differences by calculating
geometric mean estimates that were adjusted to the age distribution of the community.
• Measurement of blood, urine, and environmental PFAS concentrations in EA participants may
improve the understanding of exposure in this community but will not provide information
about all sources of exposure. Additionally, identifying every potential confounding exposure is
not possible.
• There are challenges in measurement of trace levels of PFBA in urine, including selectivity of the
analytical instrumentation and potential for external contamination. Therefore, we advise
caution when interpreting the PFBA results in urine.
• Multivariate regression models did not explain a large portion of the variability in participants’
blood PFAS levels (R-squared or R
2
, a measure of model goodness-of-fit, ranged between 0.13
and 0.30 in all-adult models). This means that other factors not identified could influence the
relationships reported in this assessment (see “Statistical Analysis” section for details).
• This EA did not directly assess participants’ tap water consumption prior to the reduction of
PFAS in the municipal water systems.
• This EA was not designed to investigate health problems associated with exposure to PFAS.
Without additional information about exposure-response relationships, the results of this EA
cannot be used to assess current or past health problems or predict the future occurrence of
disease. PFAS found in a person’s blood or urine means that exposure has occurred. The
presence of PFAS in blood or urine does not tell us how, where, when, or for how long a person

46
was exposed to PFAS. Exposure to PFAS does not mean adverse health effects will result, either
now or in the future.
• The dust results are exploratory and should be interpreted with caution. They are based on a
limited set of samples, and in some cases those samples are based on a small sample mass.
Recommendations
This PFAS EA provides evidence that past exposures to PFAS in drinking water have impacted the levels
of PFAS in people’s bodies. These PFAS are eliminated from the body over a long period of time. This
allowed ATSDR to measure PFAS even though exposures through drinking water were mitigated, or
lowered, years ago.
Although the exposure contribution from PFAS in drinking water in Security-Widefield has been
mitigated, there are actions community members and county officials can take to further reduce
exposures to PFAS and protect public health.
Based on the PFAS drinking water test results from drinking water wells in Security-Widefield, ATSDR
does not recommend an alternate source of drinking water at this time.
1. What the Security WD, Widefield WSD, and Security MHP can/should do:
a. Operators of these three public water systems should continue to monitor concentrations of
PFAS in drinking water delivered to the Security-Widefield community to ensure that
concentrations of PFAS remain below the EPA’s HA or other applicable guidelines for specific
PFAS in drinking water. Results of PFAS monitoring should be shared with community
members through appropriate communication channels (Consumer Confidence Reports for
Security WD: http://securitywsd.com/water-quality/; Consumer Confidence Reports for the
Widefield WSD, https://www.wwsdonline.com/consumer-confidence-report).
b. All treatment systems to remove PFAS from the municipal drinking water in Security-
Widefield should be maintained appropriately to ensure that PFAS concentrations remain
below the EPA’s HA or other applicable guidelines for specific PFAS in drinking water.
2. What community members can/should do:
a. Become familiar with Consumer Confidence Reports for information on water quality in
Security-Widefield (Consumer Confidence Reports for Security WD:
http://securitywsd.com/water-quality/; Consumer Confidence Reports for the Widefield
WSD, https://www.wwsdonline.com/consumer-confidence-report).
b. Private well owners living in the area affected by PFAS should consider having their wells
tested for PFAS if testing has not been conducted before. To learn more about testing wells
for PFAS visit:
https://www.elpasocountyhealth.org/news/news-release/2019/resources-
for-pfc-water-contamination-and-testing. Global public health organization NSF
International has developed a test method to verify a water filter’s ability to reduce PFOA
and PFOS to below the health advisory levels set by the EPA. NSF International-approved
devices can be found at:
https://info.nsf.org/Certified/DWTU/ Click on “reduction devices”
at the bottom of the page for PFOA and PFOS.

47
c. Nursing mothers should continue breastfeeding. Based on current science, the known
benefits of breastfeeding outweigh the risks for infants exposed to PFAS in breast milk.
d. When possible, eliminate or decrease potential exposure to PFAS in consumer products,
such as stain-resistant products and food packaging materials. To learn more visit:
https://www.fda.gov/food/chemical-contaminants-food/questions-and-answers-pfas-food
e. Pay attention to advisories about food consumption, such as local fish advisories.
f. Discuss any health concerns or symptoms with your health care provider. Share results of
PFAS blood testing with your health care provider and make them aware of ATSDR
resources for clinicians (
https://www.atsdr.cdc.gov/pfas/resources/info-for-health-
professionals.html). Follow the advice of your health care provider and the
recommendations for checkups, vaccinations, prenatal care, and health screening tests.
g. At this time, ATSDR does not have plans to conduct additional blood testing for PFAS nor
recommend PFAS EA participants get individually retested for PFAS in blood. The biological
half-lives of many of the PFAS measured in people’s blood are long. PFHxS has one of the
longest half-lives. This means that PFAS blood levels are not expected to change significantly
in the near-term, even if exposure stops. Additionally, it is unclear what an individual’s PFAS
test results mean in terms of possible health effects.
For the general population, blood tests for PFAS are most useful when they are part of a
scientific investigation like this EA. If you are concerned and choose to have your blood
tested, test results will tell you how much of each PFAS is in your blood, but it is unclear
what the results mean in terms of possible health effects. In addition, blood testing for PFAS
is not a routine test offered by most doctors or health departments. Talk to your health care
provider and make them aware of ATSDR resources for clinicians
(https://www.atsdr.cdc.gov/pfas/resources/info-for-health-professionals.html
).
h. ATSDR is funding a multi-site health study, including one site in the El Paso County area
called the Colorado Study on Community Outcomes from PFAS Exposure (CO-SCOPE). The
CO-SCOPE is being conducted by the same investigative team that completed the PFAS
AWARE study. The study will evaluate PFAS levels in serum as well as health markers and
neurobehavioral outcomes in children. If you are interested in being included in the study or
want further information, please contact
Fountain Valley PFAS Study | PFAS Multi-Site Study
Colorado: CO SCOPE (co-scope.org)
i. Follow the advice of your child’s health care provider and the recommendations for well
child checkups, vaccinations, and recommended health screening tests. Consult
https://health.gov/myhealthfinder
to help identify those vaccinations and tests. Follow the
advice of your health care provider and the recommendations for checkups, vaccinations,
and health screening tests.
j. For additional information about environmental exposures and children’s health, contact
the Pediatric Environmental Health Specialty Units, a nationwide network of experts in
reproductive and children’s environmental health (https://www.pehsu.net/
).
For More Information
If you have questions or comments or want more information on the Security-Widefield EA site, call
800-CDC-INFO or email [email protected]v. For more information on the work CDC/ATSDR is doing to address
PFAS exposure, visit ATSDR’s PFAS website: https://www.atsdr.cdc.gov/pfas/. For other EA or PFAS-
related questions, email [email protected].

48
References
This list includes references for Appendices A, B, and C, as well as the sections above.
Abraham K, El-Khatib AH, Schwerdtle T, Monien BH. 2021. Perfluorobutanoic acid (PFBA): No high-level
accumulation in human lung and kidney tissue. Int J Hyg Environ Health 237:113830. doi:
10.1016/j.ijheh.2021.113830.
[AFCEC] Air Force Civil Engineer Center. 2017. Final Site Inspection Report of Aqueous Film Forming
Foam Areas at Peterson Air Force Base El Paso County, Colorado Prepared Aerostar SES LLC, July
2017.
[ATSDR] Agency for Toxic Substances and Disease Registry. 2013. Perfluorochemical serum sampling in
the vicinity of Decatur, Alabama. Atlanta, GA. Available from:
https://www.atsdr.cdc.gov/HAC/pha/Decatur/Perfluorochemical_Serum%20Sampling.pdf
.
[ATSDR] Agency for Toxic Substances and Disease Registry. 2019a. Exposure Assessment Protocol:
Biological and Environmental Sampling of Per- and Polyfluoroalkyl Substances (PFAS), v3.0. Atlanta,
GA. Available from:
https://www.atsdr.cdc.gov/pfas/docs/pfas-exposure-assessment-protocol-
508.pdf
[ATSDR] Agency for Toxic Substances and Disease Registry. 2019b. Standard Operating
Procedures of PFAS Exposure Assessment Data Management. Version 1.3. Atlanta, GA.
[ATSDR] Agency for Toxic Substances and Disease Registry. 2021. Toxicological profile for
perfluoroalkyls. Atlanta, GA [accessed 2021 July 12]. Available from:
https://www.atsdr.cdc.gov/ToxProfiles/tp200.pdf
.
Barry V, Winquist A, Steenland K. 2013. Perfluorooctanoic acid (PFOA) exposures and incident cancers
among adults living near a chemical plant. Environ Health Perspect 121(11-12): 1313-18.
Beesoon S, Genuis SJ, Benskin JP, Martin JW. 2012. Exceptionally high serum concentrations of
perfluorohexanesulfonate in a Canadian family are linked to home carpet treatment applications.
Environ Sci Technology 46(23): 12960–7.
Buck RC, Franklin J, Berger U, Conder JM, Cousins IT, de Voogt P, et al. 2011. Perfluoroalkyl and
polyfluoroalkyl substances in the environment: Terminology, classification, and origins. Integr
Environ Assess Manag 7(4):513-41.
Calafat AM, Kuklenyik Z, Reidy JA, Caudill SP, Tully JS, Needham LL. 2007a. Serum concentrations of 11
polyfluoroalkyl compounds in the U.S. population: Data from the National Health and Nutrition
Examination Survey (NHANES) 1999-2000. Environ Sci Technol 41:2237-42.
Calafat AM, Wong LY, Kuklenyik Z, Reidy JA, Needham LL. 2007b. Polyfluoroalkyl chemicals in the U.S.
population: Data from the National Health and Nutrition Examination Survey (NHANES) 2003–2004
and comparisons with NHANES 1999–2000. Environ Health Perspect 115(11): 1596–602.
Calafat AM, Kato K, Hubbard K, Jia T, Botelho JC, Wong LY. 2019. Legacy and alternative per- and
polyfluoroalkyl substances in the U.S. general population: Paired serum-urine data from the 2013–
2014 National Health and Nutrition Examination Survey. Environ Int 131: 105048.

49
Cariou R, Veyrand B, Yamada A, Berrebi A, Zalko D, Durand S, Pollono C, Marchand P, Leblanc JC,
Antignac JP, Le Bizec B. 2015. Perfluoroalkyl acid (PFAA) levels and profiles in breast milk, maternal
and cord serum of French women and their newborns. Environ Int 84: 71-81.
Chen F, Yin S, Kelly BC, Liu W. 2017. Isomer-Specific Transplacental Transfer of Perfluoroalkyl Acids:
Results from a Survey of Paired Maternal, Cord Sera and Placentas. Environ Sci Technol 51(10):
5756-5763.
[CDC] Centers for Disease Control and Prevention. 2019. Fourth national report on human exposure to
environmental chemicals: Updated tables, January 2019, volume one. Atlanta GA [accessed 2020
June 23]. Available from: https://www.cdc.gov/exposurereport/
[CDPHE] Colorado Department of Public Health and the Environment. 2019. PFC Levels in Drinking
Water Distribution Samples Collected from the Widefield Aquifer Region. File titled: “PFC levels in
drinking water distribution samples – CDPHE.pdf”
[EPA] U.S. Environmental Protection Agency. 2019. Exposure Factors Handbook Chapter 3 (Update):
Ingestion of Water and Other Select Liquids (2019). Washington, DC, EPA/600/R-18/259F. Available
from: https://cfpub.epa.gov/ncea/efp/recordisplay.cfm?deid=343661
.
Fraser AJ, Webster TF, Watkins DJ, Strynar MJ, Kato K, Calafat AM, et al. 2013. Polyfluorinated
compounds in dust from homes, offices, and vehicles as predictors of concentrations in office
workers' serum. Environ Int. 60:128-136.
Frisbee SJ, Brooks AP, Maher A, Flensborg P, Arnold S, Fletcher T, et al. 2009. The C8 Health Project:
Design, methods, and participants. Environ Health Perspect 117(12): 1873–82.
Gluge J, Scheringer M, Cousins IT, DeWitt JC, Goldenman G, Herzke D, et al. 2020. An overview of the
uses of per- and polyfluoroalkyl substances (PFAS). Environ Sci: Processes & Impacts 22: 2345-73.
Helsel, D. 2009. Much ado about next to nothing: Incorporating nondetects in science. Ann Occup Hyg
54(3): 257–62.
[ITRC] Interstate Technology Regulatory Council. 2020. Aqueous Film-Forming Foam (AFFF). Fact Sheet.
Available from: https://pfas-1.itrcweb.org/fact_sheets_page/PFAS_Fact_Sheet_AFFF_April2020.pdf
.
Jian JM, Chen D, Han F-J, Guo Y, Zeng L, Lu X, Wang F. 2018. A short review on human exposure to and
tissue distribution of per- and polyfluoroalkyl substances (PFASs). Sci Total Environ 636: 1058–69.
Karásková P, Venier M, Melymuk L, Bečanová J, Vojta Š, Prokeš R, et al. 2016. Perfluorinated alkyl
substances (PFASs) in household dust in Central Europe and North America. Environ Int 94: 315–24.
Kärrman A, Langlois I, van Bavel B, Lindström G, Oehme M. 2007. Identification and pattern of
perfluorooctane sulfonate (PFOS) isomers in human serum and plasma. Environ Int 33(6): 782–8.
Kim K, Bennett DH, Calafat AM, Hertz-Picciotto I, Shin HM. 2020. Temporal trends and determinants of
serum concentrations of per-and polyfluoroalkyl substances among Northern California mothers
with a young child, 2009–2016. Environ Res 186:109491.

50
Kingsley SL, Eliot MN, Kelsey KT, Calafat AM, Ehrlich S, Lanphear BP, et al. 2018. Variability and
predictors of serum perfluoroalkyl substance concentrations during pregnancy and early childhood.
Environ Res 165: 247–57.
Koponen J, Winkens K, Airaksinen R, Berger U, Vestergren R, Coustins, IT, et al. 2018. Longitudinal trends
of per- and polyfluoroalkyl substances in children's serum. Environ Int (1): 591–9.
Mamsen LS, Björvang RD, Mucs D, Vinnars MT, Papadogiannakis N, Lindh CH, Andersen CY,
Damdimopoulou P. 2019. Concentrations of perfluoroalkyl substances (PFASs) in human embryonic
and fetal organs from first, second, and third trimester pregnancies. Environ Int 124: 482-492.
[NH DPHS] New Hampshire Division of Public Health Services. 2016. Pease PFC Blood Testing Program:
April 2015–October 2015. Concord, NH [accessed 2020 June 24]. Available from:
https://www.dhhs.nh.gov/sites/g/files/ehbemt476/files/documents/2021-11/pease-pfc-blood-
testing.pdf.
[NYDOH] New York Department of Health. 2019. Westhampton Beach and Quogue Area PFAS blood
testing: Group-level results. Albany, NY [accessed 2020 September 4]. Available from:
https://www.health.ny.gov/environmental/investigations/drinkingwaterresponse/docs/westhampt
on_quogue_group_level_blood_testing.
Olsen GW, Logan PW, Hansen KJ, Simpson CA, Burris JM, Burlew MM. 2003. An occupational exposure
assessment of a perfluorooctanesulfonyl fluoride production site: Biomonitoring. AIHA J 64(5): 651–
9.
[PA DOH] Pennsylvania Department of Health. 2019. PFAS Exposure Assessment Technical Toolkit
(PEATT) pilot project. Harrisburg, PA [accessed 2020 June 24]. Available from:
https://www.health.pa.gov/topics/Documents/Environmental%20Health/PEATT%20Pilot%20Project
%20Final%20Report%20April%2029%202019.pdf.
Scher DP, Kelly JE, Huset CA, Barry KM, Yingling VL. 2018. Does soil track-in contribute to house dust
concentrations of perfluoroalkyl acids (PFAAs) in areas affected by soil or water contamination?. J
Expo Sci Environ Epidemiol 29(2): 218–26.
[SGS AXYS] SGS AXYS Analytical, Ltd. 2019. Analytical Procedure for the Analysis of Per- and
Polyfluoroalkyl Substances (PFAS) in Aqueous Samples, Solids and Solvent Extracts by LC-MS/MS.
Method MLA-110 (revision 01, version 06).
Shoemaker J, Tettenhorst D. 2018. Method 537.1: Determination of Selected Per- and Polyfluorinated
Alkyl Substances in Drinking Water by Solid Phase Extraction and Liquid Chromatography/Tandem
Mass Spectrometry (LC/MS/MS). U.S. Environmental Protection Agency, Office of Research and
Development, National Center for Environmental Assessment, Washington, DC. Available from:
https://cfpub.epa.gov/si/si_public_record_report.cfm?Lab=NERL&dirEntryId=343042
Sunderland EM, Hu XC, Dassuncao C, Tokranov AK, Wagner CC, Allen JG. 2019. A review of the pathways
of human exposure to poly-and perfluoroalkyl substances (PFASs) and present understanding of
health effects. J Expo Sci Environ Epidemiol 29(2): 131-147.
https://www.nature.com/articles/s41370-018-0094-1

51
[USCB] U.S. Census Bureau. (2010). 2010 Census. Washington, DC [no date; accessed 2020] Available
from: https://www.census.gov/programs-surveys/decennial-census/data/datasets.2010.html.
Wang Y, Rogan WJ, Chen PC, Lien GW, Chen HY, Tseng YC, Longnecker MP, Wang SL. 2014. Association
between maternal serum perfluoroalkyl substances during pregnancy and maternal and cord thyroid
hormones: Taiwan maternal and infant cohort study. Environ Health Perspect 122(5): 529-34.
Wang Z, DeWitt JC, Higgins CP, Cousins IT. 2017. A never-ending story of per- and polyfluoroalkyl
substances (PFASs)? Environ Sci Technol 51:2508–18.
Watkins DJ, et al. 2013. Exposure to perfluoroalkyl acids and markers of kidney function among children
and adolescents living near a chemical plant. Environ Health Perspect 121(5): 625-30.
Wu XM, Bennett DH, Calafat AM, Kato K, Strynar M, Andersen E, et al. 2015. Serum concentrations of
perfluorinated compounds (PFC) among selected populations of children and adults in
California. Environ Res 136: 264–73.
